
The Method of Soothing the Liver in the Treatment of Acute Abdominal Pain
2019-01-24 08:18ZhngShohui張少輝YngChengcheng楊成城LiuHuiling劉會良AnJilin安佳琳CiLingling蔡玲玲RenXuewen任雪雯LiuHunwei劉歡葦
關鍵詞:楊成
Zhng Shohui (張少輝), Yng Chengcheng (楊成城)*, Liu Huiling (劉會良), An Jilin (安佳琳),Ci Lingling (蔡玲玲), Ren Xuewen (任雪雯), Liu Hunwei (劉歡葦)
aDongfang Hospital Affiliated to Beijing University of Chinese Medicine, Beijing 100078, China;
bBeijing University of Chinese Medicine, Beijing 100029, China
ABSTRACT
Pancreatic pseudocyst, whose clinical feature is small simple cyst, is a common local complication of acute pancreatitis and will not need surgery in ordinary circumstances. However, some cases could appear secondary disorders related to the location of the cyst and the role of decomposition enzymes of content, such as cyst rupture moving into the abdomen, bleeding, cystic infection, compression and internal fistula formation with adjacent organs and so on[1]. But the spleen-related complications resulting from it are rare. There was 1 patient with pancreatic pseudocyst admitted to Dongfang Hospital Affiliated to Beijing University of Chinese Medicine and the report is as follows.
KEYWORDS: Method of soothing the liver; Acute abdominal pain
MEDICAL RECORDS
A 40-year-old man was admitted to the Emergency Department of Dongfang Hospital Affiliated to Beijing University of Chinese Medicine for severe epigastric pain for 3 days. At the time of admission,there was distending pain in his midsection, radiating to the waist and back, accompanied by nausea and vomiting. No fever, chills or jaundice, no chest pain or heartburn. Besides, this patient had recurrent episodes of pancreatitis for 4 years and secondary diabetes for 3 years. His vital signs of the examination were stable, and the body temperature was normal. The respiratory sounds of lower left lung were weakened,and tenderness was obvious in midsection, especially in the left upper abdomen. His pancreas was plump and there was no signs of peritoneal irritation. Accessory examination: White Blood Cell = 26.34×109/L,NE% = 88.9%, AMY = 55.0 U/L, FPG = 9 mmol/L,vomitus occult blood (+). The results of emergency type-B ultrasonic showed that the nature of the left upper quadrant should be examined. Tentative diagnosis:1. acute attack of chronic pancreatitis and pseudocyst formation; 2. UGIH; 3. diabetes mellitus. The treatment included conventional fasting water, gastrointestinal decompression, four generation cephalosporins combined with left ornidazole against infection, intravenous nutrition, protection of gastric mucosa, inhibition of enzymes, inhibition of inflammatory mediators and fluid supplement. After the treatment above, the left upper abdominal pain was still frequent and intense, and the analgesic effect of multiple intramuscular injection of dolantin was not obvious. The results of further abdominal CT scan showed: 1. pancreatitis, and punctate calcification density in the pancreas; 2. pseudocyst in the tail of pancreas, 9.2×8.2cm, clear edge; 3. unequal density in the spleen, nonelimination of spleen infarction;4. left pleural effusion. After that, the patient developed symptoms of remittent fever and the highest temperature was 38.5 degrees. Dynamic monitoring of blood routine showed that platelet increased progressively,with a maximum value of 652×109/L, accompanied by abnormal coagulation function and D-dimer rising significantly to 4.1 mg/L. At that time, the patient was considered as pancreatic pseudocyst combined with infection but the treatment was not that effective. After 2 weeks of admission to the hospital, enhanced abdominal CT showed that there was a large pseudocyst in the tail of pancreas (as before). The coronary artery phase reformed image showed that the splenic artery and spleen were pushed to the left diaphragm. The splenic artery was located above the cyst to the back without trunk stenosis or thrombosis. However, the splenic hilar structure was in disorder; the arteries and branches were tortuous;the imaging findings were discontinuous, and the large parenchyma low density shadows of the splenic masses appeared. What showed above confirmed the diagnosis of splenic infarction. See Figure 1.

Figure1. Enhanced abdominal CT after 2 weeks of admission to the hospital showed that the arteries and branches of the splenic hilar were pressed and tortuous and the imaging findings were discontinuous (red arrows).However, the imaging findings of the splenic artery trunk were continuous and there was no blockage(the pressure at the blue arrow was narrowed by the pressure but continuous).
Considering the secondary spleen hypofunction, we used meropenem with higher potency for anti-infection on the basis of the original treatment and Pan Shengting and aspirin for anticoagulation by inhibiting platelet. At the same time, the patient complained of bitter taste, dry throat, left flank pain and obstructed defecation. He had dark purple tongue, slimy white tongue fur and taut pulse.We used the method of soothing the liver, regulating qi, purging fu and removing stasis and gave the patient Modified Dachaihu Decoction. The prescription included Bupleurum 15 g, Scutellaria baicalensis 10 g, Salvia miltiorrhiza Bge 18 g, Pinellia ternata 9 g, Rhizoma Zingiberis Recens 6 g, Ziziphus 6 g, Rehmannia glutinosa Libosch 24 g, Angelica sinensis 12 g, Cynanchum otophyllum 12 g, Curcuma zedoaria 10 g, Prunus persica 10 g, Cassia Twig 3 g, Glycyrrhiza uralensis 6 g.After seven doses, the pain was relieved and no opioid analgesics were used. Four weeks after admission to the hospital, the abdominal B-ultrasound showed that the size of the mixed hypoechoic region of the pancreatic tail was about 3.8 * 4.2cm, and the pseudocyst was considered.While the wedge-shaped hypoechoic area was found in the splenic region, it was definitely a splenic infarction.And the patient suffered from fatigue, dry mouth, and night sweats. We added Astragalus membranaceus(Fisch.) Bunge 18 g, MeLia toosendan Sieb.et Zucc. 10 g,Ophiopogon japonicus 18 g, Anemarrhena asphodeloides Bunge 10 g in the original prescription. After 6 weeks of continued treatment, the clinical symptoms of the patient were relieved. The results of the reexamination of the abdominal CT scan showed only "chronic pancreatitis,low density plaque in the spleen", and no significant cystic lesions were found in the pancreatic tail. See Figure 2. All indexes of laboratory examination were normal.After leaving the hospital, the patient was followed up for 6 months and there was no recurrence of pancreatitis or abnormal splenic function.
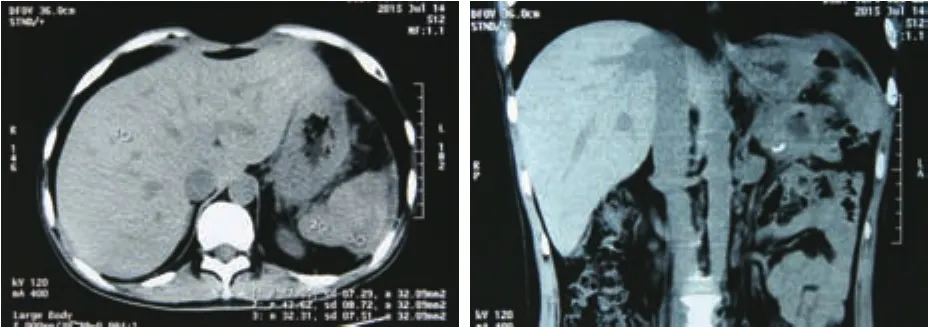
Figure 2. The reexamination abdominal of CT plain scan showed chronic pancreatitis, no obvious cyst at the tail of the pancreas, and lamellar low density shadow in the splenic parenchyma.
DISCUSSION
Due to the close adjacent relationship between the spleen and pancreas, both acute and chronic pancreatitis can lead to spleen complications, but the incidence rate is only about 2%[2]. The incidence of spleen complications associated with pancreatic pseudocysts is lower and the case reports are rare. Accetta P and other[3]found that there were no more than 50 cases retrieved by the beginning of this century. In terms of prognosis,Fishman EK and other[5]thought that once the patients with pancreatitis had spleen-related complications, the mortality rate could be as high as 50%.
The etiology of pancreatic pseudocyst complicated with splenic infarction remains unclear by now. The possible mechanism is[6-9]: 1. Pancreatitis directly invades the splenic portal or splenic vessels. 2. The pancreatic juice digests spleen parenchyma and splenic artery, which leads to aneurysm of splenic artery and thrombosis. 3.Pancreatic pseudocyst directly oppresses spleen blood vessels or spleen to cause spleen infarction. 4. In the case of pancreatitis, most of the blood vessels in the splenic portal and the spleen are in hypercoagulative state because of a high release of the high concentration of trypsin,which leads to thrombosis and microthrombus formation and causes the spleen infarction. Patients can present single or multiple complications, such as severe left upper abdominal distending pain or tearing pain, and radiating to the left shoulder, with nausea, vomiting, high fever and other typical symptoms. At present, abdominal enhanced CT, selective Celiac Arteriography and B-ultrasound have important sense to the diagnosis. In comparison,abdominal enhanced CT is a simple and effective method.The CT manifestations of typical splenic infarction show that the density of wedge-shaped infarcts in the splenic parenchyma is considerably subnormal, and there is no enhancement[5]after strengthening. Dynamic monitoring is recommended. The early diagnosis is of high value.
Combined with the imaging findings of this case,the author considered the cause of the disease as a typical giant cyst to oppress the splenic portal artery. As the branch of the splenic artery is a terminal artery lacking the rami communicans, once bent by pressure, it could lead to the relative insufficiency of the spleen bloodsupply and cause the spleen infarction, although there was no compression stenosis of the main trunk of the splenic artery. The hypercoagulative state caused by progressive increasing of the platelets after the hypofunction of the spleen could further affect the hemodynamic changes in the splenic vessels and make the spleen perfusion more inadequate and aggravate spleen infarction. After treatment, blood supply recovered and symptoms of oppression decreased as the cysts reduced. Thus, the lesion of the spleen infarction was also improved.
Rypens and others[10]thought that although the splenic complications of pancreatitis caused obvious pathological changes, 75% would be self-cure, only 12.1% would be unstable and need splenectomy.However, the mortality and incidence rate of postoperative complications of surgical treatment of splenic infarction and splenic subcapsular fluid are higher.Therefore, we tend to perform non-surgical treatment.Most scholars believe that surgery should emphasize not only the remedy of splenic complications, but also the treatment of the disease of pancreatitis itself[11].
Traditional Chinese medicine has obvious advantages in term of treating of acute pancreatitis and its common complications. In recent 30 years, the basic and clinical studies based on Dachaihu Decoction have confirmed that it has a definite effect on inhibiting the release of pancreatic enzymes and excessive activation of inflammatory mediators, controlling infection and improving the microcirculation of the pancreas, which provides higher efficacy and better patient compliance than the treatment of Western medicine and shortens the time of hospitalization[12]. According to the characteristics of this patient's symptoms, bitter taste, dry throat, left flank limb spasm, distending pain that seemed to be feeling of fullness and dull pain in the upper abdomen(distress below the heart), and constipation were typical indicatoins of Dachaihu Decoction. The tongue was purple and dark and with a white and greasy coat and the pulse was wiry, which we considered as syndrome of dampness retention in middle-energizer, stagnation in Shao-yang,obstruction of zang and fu and collaterals. The wiry pulse represents the liver and pain. Therefore, Bupleurum and Scutellaria baicalensis were used to relieve qi stagnation of liver and reconcile Shao-yang, and a large number of Salvia miltiorrhiza Bge and Rehmannia glutinosa Libosch were used to cool blood and dissipate blood stasis and to tonify internal deficiency and to promote and ascend qi. And Angelica sinensis and Cynanchum otophyllum were used to nourish blood and soothe the liver and Curcuma zedoaria to promote flow of qi and remove stagnation. Besides, Cassia Twig could help Cynanchum otophyllum to promote blood circulation and regulate the nutrient qi. In the later period, the characteristic of dredging and moving rapidly of MeLia toosendan Sieb.et Zucc was used to to strengthen the effect of activating qi and blood circulation to remove stasis. Astragalus membranaceus (Fisch.) Bunge, Ophiopogon japonicus and Anemarrhena asphodeloides Bunge could tonify qi and yin to avoid dissipating qi and injuring the vital qi by the above medicine. The whole prescription strengthened body resistance and eliminated pathogenic factors,addressed both the symptoms and root cause, embodied that unobstructed qi and blood circulation can remove the pain, provided outlet for the pathogenic factors and removed the stasis to produce the fresh blood. Finally,the pancreatic pseudocyst was absorbed and the splenic infarction was significantly relieved. Animal studies have shown that[24]Salvia miltiorrhiza Bge has an important protective effect on the immune function of the spleen in the improvement of acute severe pancreatitis. It can also effectively improve the pancreatic microcirculation and play a two-way regulatory role in blood coagulation dysfunction, regulate immune factors, inhibit excessive release of inflammatory mediators, and clean up serum endotoxin and phospholipase A2 to protect organ function and therefore improve prognosis and promote recovery.
In summary, the number of reports of splenic complications associated with pancreatitis and pancreatic pseudocyst are increasing year by year, but they are still rare. In term of anatomy, the cognition of this disease is relatively consistent. However, there is no large sample of clinical and basic research to confirm the pathogenesis. Most of them are theoretical analysis and lack of evidence-based basis. In recent years, the mechanism of traditional Chinese medicine treatment of acute pancreatitis has been studied extensively and deeply and its clinical efficacy and the significance of health economics have gained affirmation. But the relevant research is still not rigorous in term of methodology,and there is heterogeneity and potential bias between studies[14]. Hence, we need to design a number of more scientific and reasonable multicenter randomized studies to confirm it, which deserves surgical clinical attention.
猜你喜歡
上海師范大學學報·自然科學版(2022年3期)2022-07-11
延河(2018年5期)2018-06-11
試題與研究·高考理綜物理(2016年3期)2017-03-28
試題與研究·高考理綜物理(2016年3期)2017-03-28
中學生數理化·高一版(2016年6期)2016-05-14
微型小說選刊(2014年23期)2014-05-18
當代教育(2009年4期)2009-05-19
作文大王·低年級(2008年8期)2008-09-03
雕塑(1999年2期)1999-06-28
雕塑(1997年2期)1997-06-30
 World Journal of Integrated Traditional and Western Medicine2019年1期
World Journal of Integrated Traditional and Western Medicine2019年1期
- World Journal of Integrated Traditional and Western Medicine的其它文章
- World Integrated Medicine Master Wu Yiling
- Evaluation of Efficacy and Safety of Electro-acupuncture Precondition on Postoperative Cognitive Dysfunction (POCD)Following Knee Replacement in Elderly:A Randomized Controlled Trial
- New Year's Message
- Effects of Acupoint Massage Combined with Psychological Nursing on Depression and Hope Level and Coping Style in Hospitalized Patients with Hepatocirrhosis
- Effects of Yigan Tiaozhi Decoction on Serum NO, Endotoxin and RBP4 in Patients with Nonalcoholic Fatty Liver Disease
- Clinical Comparison and Analysis of Decoction of Traditional Chinese Medicine Combined with Ear Acupoint Application and Simple Artificial Tears in the Treatment of Dry Eye Syndrome