
Effectiveness of animal-assisted therapy on pain in children:A systematic review and meta-analysis
2021-02-28 09:48YuanyuanZhangFanghongYanSijunLiYutanWangYuxiaMa
Yuanyuan Zhang,Fanghong Yan,Sijun Li,Yutan Wang,Yuxia Ma
Evidence-Based Nursing Center,School of Nursing of Lanzhou University,Lanzhou,Gansu,China
Keywords:Animal-assisted therapy Children Meta-analysis Pain Systematic review
ABSTRACT Aims:Animal-assisted therapy(AAT)relieves pain by creating a relaxed and comfortable environment to reduce anxiety in children.Yet little is known about its effects on pain in children.This study aims to systematically evaluate the effects of AAT on pain in children.Methods:Eight databases including PubMed,Cochrane Library,Web of Science,CINAHL Complete,Chinese Biomedical Database(CBM),Weipu Database(VIP),China Knowledge Resource Integrated Database(CNKI) and Wanfang Database were retrieved,and all randomized controlled trials or controlled clinical trial using AAT on children’s pain were recruited from inception to October 2019.Two reviewers independently screened literature,extracted data and assessed the risk of bias of the included studies.RevMan 5.3 software was employed for meta-analysis.Results:Seven published studies containing 4 RCTs and 3 CCTs were included for the systematic review.The results of meta-analysis showed that AAT could reduce children’s pain when compared with the control group [MD=-0.53,95% CI (-0.77,-0.30),P < 0.00001].Conclusion:Current evidence shows that AAT can relieve pain in children to some extent.Considering the limited quality and quantity of the available studies,more high quality studies should be performed to verify the above conclusion.
What is known?
·Current clinical guidelines cover acute operational pain,postoperative pain,and chronic pain.
·The recommendations of the clinical practice guidelines mainly involve 8 aspects of pain management in children,including pain-causing operation,expression pattern of pain,principles of pain management,participants,pain assessment,intervention,records and training.
·Benefits of exposure to animal companion to human health,both in physical and psychological aspects,have been welldocumented.
·Animal-assisted therapy(AAT)has now been applied frequently in psychological disorders among children,such as autism,depression,attention deficit disorder,and a favourable therapeutic effect has been documented.
What is new?
·The evaluation results of this system showed that AAT could reduce children’s pain.
·AAT could also reduce children’s the degree of behavioral distress to some extent,and influence the respiratory rate,heart rate,diastolic blood pressure,oxygen saturation and cerebral oxygenation in children,but could not significantly improve the anxiety level of children and their parents.
1.Introduction
Pain,an unpleasant subjective sensory and emotional experience with existing and potential tissue damage [1],is listed as the fifth most important vital sign after body temperature,pulse,respiration and blood pressure [2].Pain experience of children is easily neglected [3],and incidence of pain is especially higher among hospitalized children [4].Studies have shown that chronic pain in children can cause anxiety,depression and other negative emotions,seriously affecting their quality of life[5,6].Despite this,there is a lack of effective pain management model for children among existing studies.
The multi-mode analgesic administration regimens (such as aspirin,non-aspirin,paracetamol,etc.) are commonly adopted clinically to relieve pain in patients.However,opioids may still cause adverse reactions such as nausea,vomiting,respiratory depression and hallucination for patients,even though its dose has been reduced [7-9].Therefore,non-drug therapies,such as music therapy,cognitive behavioral therapy and animal assisted therapy(AAT),are preferred by healthcare staff and patients due to their minimal side effects and easy implementation.Among them,the application of AAT,as one of the non-drug intervention methods dealing with children’s pain,is gradually increasing [10-13].Animal-assisted therapy (AAT) is different from common interaction with companion animals.AAT,also known as animal-assisted intervention,is a conscious and unique form of therapy involving the patient,trained animal and human owner or trainer as a therapist,with the aim of promoting the patient’s success in achieving therapeutic goals.Such goals can include improvement in physical,social,emotional,and cognitive functioning [14-18].AAT relieves pain by creating a relaxed and comfortable environment to reduce anxiety in children[10,12].
So far,majority of studies have indicated the effectiveness of AAT in improving and managing the clinical outcomes of pain in children,yet there is still a shortage of robust evidence and its practicability is controversial.Therefore,this study,as the first meta-analysis focusing on summarizing the effectiveness of AAT on pain in children through reviewing previous studies,aims to evaluate its effectiveness for pain management,and provide theoretical basis for reducing the pain of children in the methods of systematic review and meta-analysis.
2.Methods
2.1.Search strategy
Eight electronic databases,i.e.PubMed,Cochrane Library,Web of Science,CINAHL Complete,Chinese Biomedical Database(CBM),Weipu Database (VIP),China Knowledge Resource Integrated Database(CNKI)and Wanfang Database,were searched for articles that evaluated AAT on children’s pain,and were published from the database’s inception to October 2019.We also checked the reference lists of relevant articles for additional studies,utilizing backward and forward searching for relevant articles.The search terms of the MeSH and free text terms included Child/Children/Infant/Nurseling/Adolescent/Teen/Teenager/Youth/Pediatric/Neonate/Toddler/Minors/animal assisted therapy/animal facilitated therapy/pet facilitated therapy/DAT/AAT/pet therapy/animal assisted intervention/animal assisted activity/animal therapy/animal-assisted therapy/animal-assisted activity/AAA/animal-assisted intervention/pet-therapy intervention/animal-facilitated therapy.Appendix A provided the search strategies for all the databases,which used a combination of MeSH and free text terms.The search ensured that MeSH terms were exploded.Free text terms were searched in the title,abstract,summary,heading or keywords.The search strategy was adjusted as appropriate for each database retrieved.
2.2.Eligible criteria
Studies were included when the following criteria was met:(a)Randomized controlled trial(RCT)or controlled clinical trial(CCT);(b) Age range:3-18 years (regardless of race,nationality,type of disease,or course of illness); (c) In the experimental group,the intervention was conducted in the way of AAT,in which the animal was introduced into the ward as a therapist and had close interaction with the children; Other treatments were used in the control group,such as jigsaw puzzles,basic post-operative medical care,or parental care; (d) The main outcome measures were pain intensity score,measured by Numeric Rating Scale (NRS),Facial Pain Scale(FACS)and Visual Analogue Scale(VAS),PedsQL Present Functioning Scales; (e) Secondary outcome measures were physiological,anxiety,and behavioral distress,including diastolic blood pressure,heart rate,respiratory rate,oxygen saturation,and cerebral oxygenation.
Studies which met the following criteria were excluded:(a)Repeated publications; (b) Non-Chinese and English literature; (c)Without related outcome measures; (d) Conference papers; (e)Literature with incomplete data that cannot be extracted.
2.3.Study selection
Two reviewers independently screened the literature,extracted the data and cross-checked them.In the event of disagreement,a third reviewer adjudicated.In the process of literature screening,the title of the text is read first.After excluding the obviously irrelevant literature,the abstract and full text are then read to determine whether the literature should be included.Where necessary,the original study author was contacted by email or phone for undetermined but important information for the study.
2.4.Data extraction and quality appraisal
Two experienced reviewers independently extracted data of interest using a standard electronic form which were checked for agreement prior to data analysis.Disagreements regarding data extraction were resolved through discussion.The extracted data included patient and study characteristics,including sample size,treatment comparisons,pain score of each group.If these data were not reported,we contacted the corresponding author to obtain data.
Two reviewers evaluated the risk of bias among the included RCT and CCT literatures respectively according to the evaluation criteria of Cochrane Systematic Review Manual 5.1.0 [19]and JBI 2005 [20].The evaluation items of Cochrane Handbook 5.1.0 included:random sequence generation,allocation concealment,blinding,incomplete outcome data,selective reporting and other sources of bias.Each study was assessed as either“low risk of bias”,“high risk of bias”,or “unclear risk of bias” for each item based on study reporting and/or additional information provided by the study authors;JBI 2005 included 9 items,mainly evaluates whether the study has the characteristics of causal relationship,baseline comparability,control group,loss of follow-up of the study object,result evaluation method and data analysis method.According to above criteria,“yes”,“no”,“unclear”or“not applicable”are used to evaluate the included CCT literature one by one.After independent evaluation,two reviewers discussed and reached a consensus.If there was any disagreement,the third reviewer would arbitrate or the research group would decide.
2.5.Data analysis
RevMan5.3 software was applied for statistical analysis.Mean difference (MD) was regarded as the effect analysis statistic for measurement data,and risk ratio (RR) was used as the effect analysis statistic for dichotomous variables.95%CI was provided for each effect.Heterogeneity among the included studies was quantitatively determined by c2test of heterogeneity and the I2statistic.If there was no statistical heterogeneity among the results,fixedeffect model was used for meta-analysis.If there was statistical heterogeneity among the results,the source of heterogeneity was further analyzed.After excluding the influence of obvious clinical heterogeneity,random effect model was used for meta-analysis.Significant clinical heterogeneity was treated with subgroup analysis or sensitivity analysis.All P values were calculated from two tailed tests of statistical significance with a type I error rate of 0.05.
This systematic review does not require ethical assessment because only indirect literature will be included and evaluated.
3.Results
3.1.Literature selection
The literature search identified 2,375 studies,of which 272 were duplicates.A further 2,053 studies were excluded after the initial screening of titles and abstracts.The full-text of the remaining 50 studies was further reviewed,of which 7 were considered eligible for this review(Fig.1).
3.2.Study characteristics and risks of bias
Table 1 summarized the main characteristics of the seven studies [10,12,13,21-24],which included the authors,publication date,study location,sample size,sex distribution,mean age,sample size,interventions,intervention time,outcome indicators and pain assessment tool.There were 4 RCT studies and 3 CCT studies.These studies were performed in USA(4 studies),Italy(1 study)and Brazil(2 studies).The duration of intervention ranged from 10min to 16 h.
The final methodological quality evaluation of the 7 included studies was shown in Table 2 and Table 3.The quality evaluation grade of the literature was above medium.And there were no statistically significant differences in age,gender and other aspects between the included experimental group and the control group,and baseline data were comparable.
3.3.Meta-analysis
3.3.1.Pain
Pain was reported in 7 trials [10,12,13,21-24],including 4 RCTs and 3 CCTs.The NRS,FACS and VAS were used to measure the pain degree in these studies.In the subgroup analysis of study types,both the RCT group[SMD=-0.44,95%CI(-0.75,-0.12),P=0.007]and the CCT group[SMD=-0.66,95%CI(-1.01,-0.31),P=0.0002]showed that AAT could alleviate children’s pain.There was no statistically significant difference between the results of RCTs and CCTs(χ2=0.85,P=0.36).The results of meta-analysis showed that AAT could reduce children’s pain when compared with the control group[MD=-0.53,95% CI (-0.77,-0.30),P <0.00001](Fig.2).
3.3.2.Physiological indicators
Three studies[10,12,23]reported the effects of AAT on diastolic blood pressure and heart rate.Results of meta-analysis in fixedeffect models showed there was no statistical difference in diastolic blood pressure between the experimental group and the control group[MD=-2.88,95%CI (-6.03,0.28),P=0.07](Fig.3).Since there was no significant heterogeneity among studies(P=0.24,I2=29%),the fixed-effect model was used to analyze the effect of AAT on heart rate.Results of meta-analysis indicated that there was no statistical difference in heart rate between two groups[MD=5.61,95%CI (-0.77,11.99),P=0.08](Fig.4).Only one study found [10]the respiratory rate of experimental group was slightly higher than that of control group(t=-2.63,P=0.011),while the difference of pulse between the two groups was not statistically significant.Calcaterra [12]showed that there were certain differences in the time distribution of oxygen saturation and cerebral oxygenation between groups.At the beginning of the observation period,the difference of oxygen saturation was the highest among groups.But in the later observation period,the experimental group brain oxygenation had the tendency to increase.
3.3.3.Anxiety
Three studies [21-23]reported anxiety levels of parents and children.Subgroup analysis was performed according to different objects.Two studies [22,23]mainly assessed the anxiety level of parents.Meta-analysis of the random-effect model showed that there was no statistically significant difference in the anxiety level between the experimental group and the control group[MD=-0.10,95%CI(-0.70,0.51),P=0.75]; Two studies [21,24]assessed the anxiety level of children,and meta-analysis of the random-effect model showed that there was no statistically significant difference in the anxiety level between the two groups[MD=-0.38,95%CI(-0.80,0.05),P=0.08](Fig.5).

Table 1 Characteristics of the included study.

Fig.1.Flow chart of the literature search and selection process.


Table 2 Methodological quality evaluation of randomized controlled trials.

Table 3 Methodological quality evaluation of controlled clinical trial.

Fig.2.Forest plot of comparison between the experiment group and the control group regarding to pain score.

Fig.3.Forest plot of comparison between the experiment group and the control group regarding to diastolic blood pressure.
3.3.4.Behavioral distress
Only one study [22]reported the degree of behavioral distress between experimental group and control group.Study of Vagnoli[22]showed the total degree of behavioral distress in the AAT group was lower than that in the control group(MD=8.87,P=0.042).
4.Discussion
4.1.Principal findings of this review
This study was based on the 7 study literatures included in the current meta-analysis,which involved a total of 236 patients.And the quality evaluation grade of the literature is above medium.The results of this study showed that AAT could relieve children’s pain,reduce the degree of behavioral distress to some extent,and change the respiratory rate,heart rate,diastolic blood pressure,oxygen saturation and cerebral oxygenation of children,but could not significantly improve the anxiety level of children and their parents.
4.2.Pain
Studies have shown that 15%-20%of children have experienced chronic pain,40%of children undergoing surgery have experienced moderate or severe pain,and 75% of children’s postoperative pain has not been effectively controlled[25].Repeated painful stimuli in the early stages of life can lead to acute stress,permanent damage to the central nervous system and emotional disorders [7].The results of this study show that AAT can relieve pain in children,which is similar to previous findings [26].Analysis of its possible mechanism of action includes:On the one hand,children can be distracted by spending time with animals,and distraction is one of the most effective ways to control and relieve pain [12]; On the other hand,animals also provide social support for humans.The spontaneous interaction and pleasure between humans and animals make both sides feel happy and warm.This harmonious and joyful atmosphere is needed for treatment.When touching and hugging animals,it can make children feel warm inside,meet the need of physical contact,stabilize emotions and reduce the pain of children[12,15].Additionally,AAT can regulate the neuroendocrine reaction of the human body.In this reaction,emotions can promote the biochemical mediated nerve and immune response,causing the release of endorphins,producing a feeling of happiness and can increase its immune response[27,28].Therefore,AAT has a positive role in promoting pain relief in children.
4.3.Physiological indicators
Results of this study showed that there were no statistically significant differences in diastolic blood pressure,respiratory rate,heart rate or pulse in patients with AAT.However,there was an overall trend of decrease which may be related to the small sample size of the included study,suggesting that physiological indicators can objectively detect the physiological responses of the endocrinological and autonomic nervous systems related to pain,and AAT may improve the pain of the children to influence their related physiological indicators [29].The results of this study need to be further confirmed by future high quality studies with larger samples.Studies have shown that animal support activates emotional areas of the brain,including parts of the limbic system and prefrontal cortex,which can influence breathing,heart rate and diastolic blood pressure in children [30].Other studies [22,23,31,32]have found that bringing animals into pediatric wards can increase the participation of hospitalized children and improve the satisfaction of their parents and medical staff.Furthermore,nosocomial infection rate did not change.
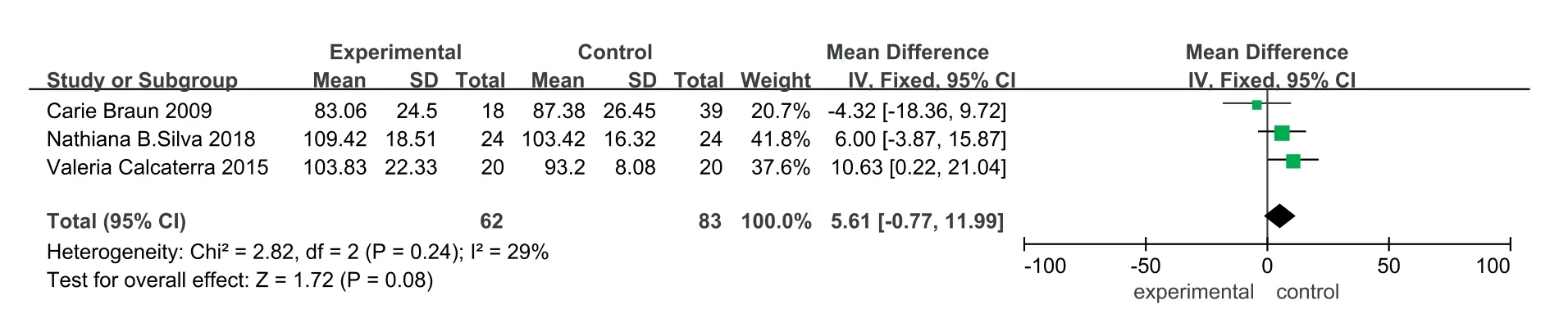
Fig.4.Forest plot of comparison between the experiment group and the control group regarding to heart rate.

Fig.5.Forest plot of comparison between the experiment group and the control group regarding to anxiety.
4.4.Anxiety
Anxiety or distress can heighten the perception of pain.Further,more anxious children report higher levels of pain[33].Therefore,it is important to reduce children’s anxiety.The results of this study showed that AAT did not significantly reduce the anxiety level of both in children and their parents.On the one hand,the short intervention duration couldn’t establish stable effect,thus may not indicate significantly statistical result; on the other hand,the baseline level of anxiety in the AAT group was lower than that in the control group,which may reduce the potential ability to identify the change of anxiety.Qualitative research results also found that AAT can reduce the behavioral distress degree of children to a certain extent,so that children can get comfort and satisfaction,which is consistent with the research results of Hansen[34].It may be that animals attract a portion of children’s attention away from their own negative environment and toward their interactions with animals,thereby reducing their behavioral distress.
5.Strengths and limitations
This study is of some advantages,including a comprehensive search,careful quality assessment and a rigorous quantitative comprehensive approach.However,this study has limitations.Firstly,only Chinese and English literatures are included,so there is the possibility that those published in other languages that meet the inclusion criteria have not be included.Secondly,due to the heterogeneity of outcome indicators,including different data formats or study objects,some results may not be quantifiable.Thirdly,the number of RCTs and CCTs included was small.Thus,new clinical studies should be included in the future to update the research conclusions.The above limitations may affect the demonstration strength of the system evaluation.In order to obtain more objective conclusions,subsequent studies should pay more attention to the rigor of the research design while increasing the sample size,determining the nature of the subjects’pain,the type of disease,and the duration of the AAT intervention,so as to improve the research quality.
6.Conclusions
In conclusion,this systematic review found that AAT could reduce children’s pain,reduce children’s behavioral distress degree to a certain extent,and influence their respiratory rate,heart rate,diastolic blood pressure,oxygen saturation and cerebral oxygenation.As a non-drug intervention method,AAT has a certain effect in alleviating pain in children and is relatively safe,make it practicable for promotion among children patients.However,the development and application of Chinese AAT is in its infancy.Due to the lack of professionals,insufficient research evidence,and the prohibition of carrying animals in hospitals and other places,AAT has not been widely promoted in China at present,which needs further exploration by researchers.And relevant medical facilities can also try to relax the regulations and introduce animals as therapists into the clinic,so as to verify the application effect of AAT.
Funding
National Nature Science Foundation of China (grant No.71704071).
CRediT authorship contribution statement
Yuanyuan Zhang:Software,Data curation,Writing -Original draft preparation.Fanghong Yan:Formal analysis,Methodology.SijunLi:Software,Validation.Yutan Wang:Visualization,DataCuration.Yuxia Ma:Conceptualization,Writing-Reviewing and Editing.
Declaration of competing interest
The authors declare that they have no competing interests.
Appendices.Supplementary data
Supplementary data related to this article can be found at https://doi.org/10.1016/j.ijnss.2020.12.009.
 International Journal of Nursing Sciences2021年1期
International Journal of Nursing Sciences2021年1期
- International Journal of Nursing Sciences的其它文章
- Focuses and trends of the studies on pediatric palliative care:A bibliometric analysis from 2004 to 2018
- Relationship between negative emotions and perceived support among parents of hospitalized,critically ill children
- The effect of digital health technologies on managing symptoms across pediatric cancer continuum:A systematic review
- Effects of creative expression program on the event-related potential and task reaction time of elderly with mild cognitive impairment
- Struggling to live a new normal life among Chinese women after losing an only child:A qualitative study
- Implementation and evaluation of a pain management core competency education program for surgical nurses