
Main Renal Artery Plus Branch Ablation in the Treatment of Resistant Hypertension with Renal Denervation
2021-06-08 01:47TinJioLyuLingYnLiXuWngJinYeJunQingGondZongJunLiu
Tin-Jio Lyu , , Ling-Yn Li , , Xu Wng , Jin Ye , Jun-Qing Go nd Zong-Jun Liu
1 Department of Cardiology, Putuo Center Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, 200062 Shanghai, People’ s Republic of China
Abstract Objective: To study the safety and efficacy of denervation of renal artery branches in the treatment of resistant hypertension.Methods: Sixty patients with resistant hypertension were enrolled.The patients were randomly assigned to the main renal artery plus branch ablation group or the main renal artery ablation group.The clinical data and operation-related parameters, including number of ablation points, temperature, and average energy, were recorded.Ambulatory blood pressure was taken for all patients at the baseline and at 6 months after treatment.Office blood pressure was recorded before treatment and after treatment every 3 months for 2 years.Results: Sixty patients with resistant hypertension were enrolled in this study.There were 30 patients in each group.Angiography was performed after ablation.No renal artery complications, such as stenosis and dissection, occurred in the two groups.There was no significant difference in age, sex, BMI, comorbid disease, and medication between the two groups (P > 0.05).The number of ablation points for the main renal artery plus branch ablation group was greater than that for the main renal artery ablation group.The office blood pressure and 24-hour blood pressure were significantly lower 6 months after treatment than before treatment in both groups (P < 0.05).Office blood pressure in the main renal artery plus branch ablation group was lower than that in the main renal artery ablation group during the 3- 12-month follow-up period, with a statistical difference.However, as the follow-up time increased, the difference disappeared.Conclusion: The results of this study show that main renal artery plus branch ablation is a safe interventional method,but there was no obvious advantage on long-term follow-up compared with only main renal artery ablation.
Keywords: Renal denervation; resistant hypertension; percutaneous renal artery sympathetic nerve ablation
Introduction
Catheter-based renal denervation (RDN) is a new technology developed in recent years to treat resistant hypertension, which is a focus of modern medicine.Symplicity HTN-1, Symplicity HTN-2,and other clinical studies showed that RDN can effectively reduce blood pressure in patients with resistant hypertension [1 - 3].However, a multicenter, prospective, single-blind, randomized controlled trial in 2014, Symplicity HTN-3, showed no significant antihypertensive effects of RDN in resistant hypertension [4]; therefore, the effectiveness of blood pressure control methods has been controversial.Some problems with research remain, such as the operation technique and defective intervention devices.The subsequent Global Symplicity Registry included 1000 patients and found that RDN can safely and effectively reduce overall blood pressure in patients with resistant hypertension [5].However, whether RDN has better antihypertensive effects than other surgical or ablative methods is unclear.Moreover, whether device improvement plays a decisive role in treatment requires further clinical trials for verification.Improvement of interventional techniques also plays an important role in the treatment of RDN.A subgroup analysis of the SPYRAL study [6] suggests that main renal artery plus branch ablation has a better antihypertensive effect than only main renal artery ablation at 6 months after the RDN procedure.This prospective, randomized controlled study further investigated the long-term effect of main renal artery plus branch ablation over 2 years after the RDN procedure compared with only main renal artery ablation.
Methods
Study Design
This trial was a single-center, prospective, randomized controlled trial.It was approved by the Ethics Committee of Putuo Hospital and conducted in accordance with the Declaration of Helsinki and good clinical practice guidelines.All patients provided written informed consent before randomization.
Patients
The inclusion criteria were as follows:
? Patients aged 18- 80 years with diagnosed resistant hypertension.
? Patients taking three or more antihyper tensive medications, including one diuretic, who had not yet achieved blood pressure control(> 140/90 mmHg), referred to as resistant hypertension [7- 10].These patients were given losartan hydrochlorothiazide and amlodipine for at least 4 weeks, then patients have still not yet achieved blood pressure control.
The exclusion criteria [11] were as follows:
? Patients with a history of renal artery stenosis or imaging suggestive of renal artery stenosis.
? Glomerular filtration rate less than 45 mL/min/1.73 m2.
? Type 1 diabetes.
? Severe valvular heart disease.
? Pregnant or planning to become pregnant during the study.
? Myocardial infarction or cerebrovascular accident within the previous 6 months.
? Diameter of the renal artery branch less than 2 mm.
Research Group
The randomized envelope method was used in this study.After renal artery angiography, patients were randomly divided into the main renal artery plus branch ablation group and the main renal artery ablation group.
RDN Intervention
Patients were given 300 mg aspirin or 300 mg clopidogrel and intraoperatively heparin (6000- 8000 U).On the right side of the groin, the skin was prepared and disinfected, the femoral artery was punctured, and a 7 F vascular sheath was inserted.Left and right renal artery angiography was performed with a JR4 catheter, and a 7 F LIMA catheter was implanted in the left and right renal arteries.A 6 F microcirculation renal artery radiofrequency ablation catheter was placed in the left and right renal arteries in temperature control mode at 6- 15 W,43 ° C, with an ablation instrument (39D-72X,Johnson Medical Instrument Co.Ltd.).Each point had an effective ablation time of 60 seconds for the left and right renal artery ablation (four to six points for each ablation).The main renal artery plus branch ablation group also needed ablation of one to three points per branch.Renal artery angiographs were reviewed after ablation in both groups.
Drug Adjustment Plan
Initial oral antihypertensive drugs were recorded for all patients according to the type and number of conventional antihypertensive drugs.During the follow-up period, it was recommended to add drugs if systolic blood pressure was greater than 160 mmHg or diastolic blood pressure was greater than 100 mmHg for the previous 3 days; it was advisable to reduce the dose if systolic blood pressure was less than 90 mmHg and/or diastolic blood pressure was less than 60 mmHg.
Study Evaluation
Patients were followed up for 24 months.The following data were collected and analyzed:
? Basic data, including sex, age, comorbid disease,and medication.
? Operation-related parameters, including ablation points, temperature, and average energy.
? Ambulatory blood pressure before treatment and 6 months after treatment.The ambulatory blood pressure monitoring time was from 6:00 to 21:59 for daytime and from 22:00 to 5:59 for nighttime.Measurements were performed per 30 minutes during the day and per hour during the night.Patients were told to avoid strenuous exercise during the monitoring.
? Office blood pressure, monitored every 3 months.
Statistical Analysis
All data were statistically analyzed by IBM SPSS Statistics version 22.0.Normally distributed measurement data are expressed as the mean ± standard deviation.The independent samplesttest was used to compare the two groups.The pairedttest was used to compare the two groups before and after treatment.Repeated measurement data were assessed by multiple-factor analysis of variance.Comparison was performed with the Wilcoxon rank-sum test.Counting data were evaluated by the chi-square test.
Results
Baseline Data
This study included 60 patients with resistant hypertension in our center from 2015 to 2018.The main renal artery ablation group and the main renal artery plus branch ablation group each had 30 patients.After ablation we checked the angiographs, and found that no renal artery complications, such as stenosis and dissection, had occurred in the two groups.Only one patient in the main renal artery ablation group was lost to follow-up; the remaining 59 patients completed 2 years of follow-up.There was no significant difference in age, sex, BMI,comorbid disease, and medication between the two groups (P > 0.05) (Table 1).Antihypertensive drugs did not change in the two groups before and after treatment.
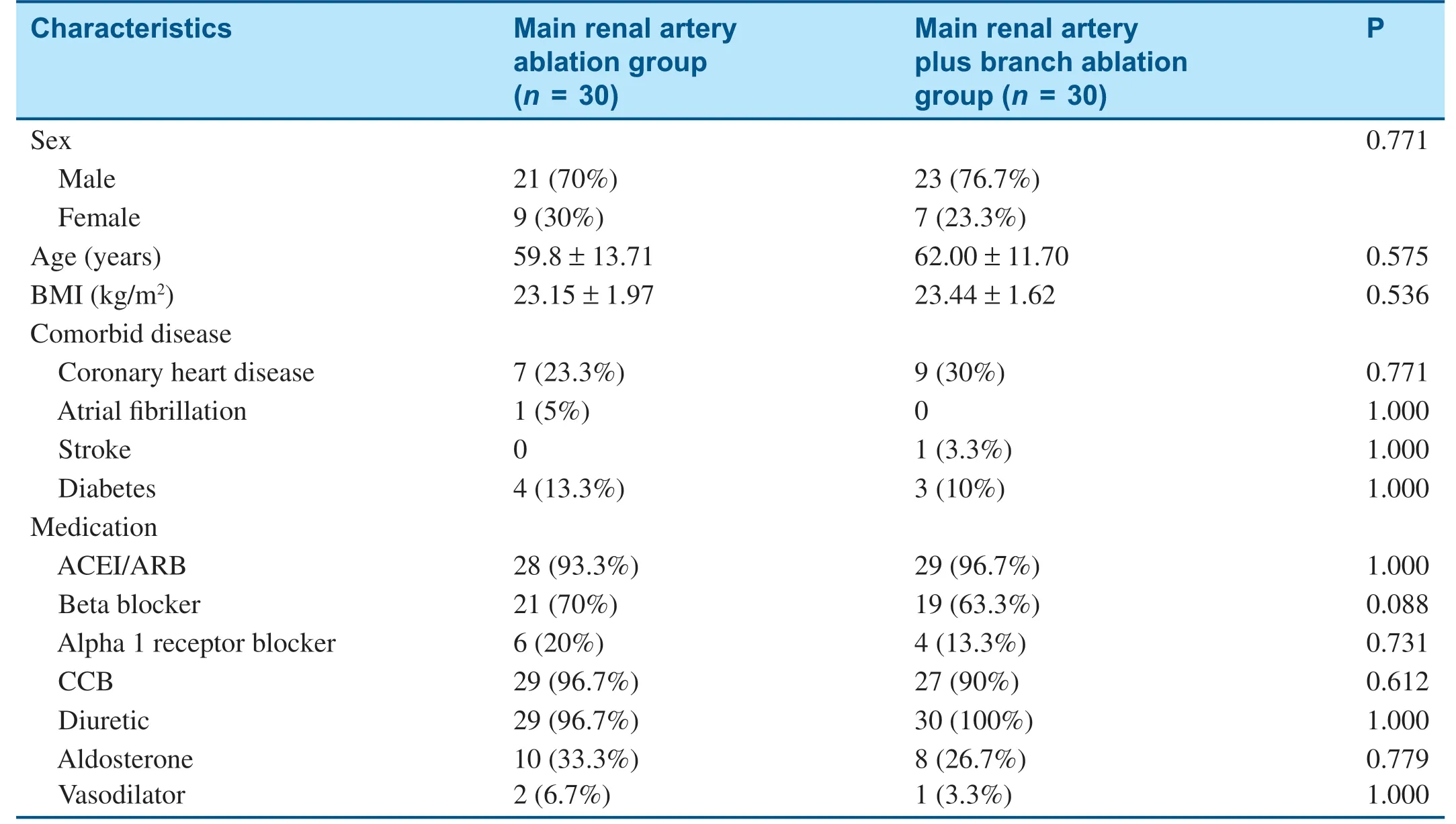
Table 1 Baseline Characteristics of Patients.
Ablation Parameters
Ablation was performed in the two groups of patients according to the protocol.The results of the ablation are shown in Table 2.The number of ablation points for the main renal artery plus branch ablation group was significantly greater than for the main renal artery ablation group.There was no significant difference between the two groups in the ablation temperature.In the main renal artery plus branch ablation group the difference between postoperative and preoperative impedance parameters was significantly greater than in the main renal artery ablation group, and the average energy was significantly lower than in the main renal artery ablation group (P < 0.05).

Table 2 Ablation-Related Parameters.
Efficacy
Compared with before treatment, after treatment there was a significant decrease in the 24-hour bloodpressure in the two groups (P < 0.05) (Table 3).We found the blood pressure in the clinic of the main renal artery plus branch ablation group was lower than that of the main renal artery ablation group during the 3- 12-month follow-up period, with a statistical difference.However, as the follow-up time increased, the difference disappeared.As Figures 1 and 2 show, the systolic blood pressure in the clinic of the main renal artery plus branch ablation group was lower than that of the main renal artery ablation group during the 3- 12-month follow-up period,with a statistical difference.There was no significant difference between the two groups during the 15- 24-month follow-up period.
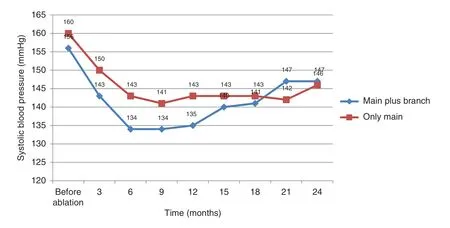
Figure 1 Follow-up of Systolic Blood Pressure in the Two Groups.
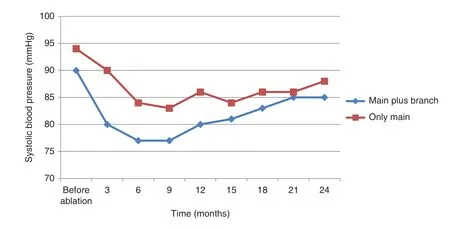
Figure 2 Follow-up of Diastolic Blood Pressure in the Two Groups.

Table 3 Ambulatory Blood Pressure (mean ± standard deviation) in Both Groups (mmHg).
Discussion
The sympathetic nervous system plays an important role in the development of hypertension [12].Renal sympathetic efferent nerves can decrease renal blood flow, decrease urinary excretion of salt and water, and increase renin release fromthe kidney [13].Percutaneous renal artery sympathetic nerve denervation is a new technology developed in recent years to treat resistant hypertension.It might lower blood pressure by reversing these mechanisms.Clinical trials [14- 18] showed that RDN can effectively reduce intractable blood pressure in hypertensive patients.This study is a prospective, randomized controlled study, and the results also show that RDN can significantly reduce patient blood pressure.Although controversy has been raised about the validity of the negative results of RDN in the treatment of resistant hypertension in the Symplicity HTN-3 study [4], RDN intervention cannot be overlooked.In the Symplicity HTN-3 study there were many problems, including too many centers involved, fewer cases of singlecenter enrollment, a single catheterization system,single equipment, and fixed setup parameters.The lack of previous RDN intervention experience in participating centers may not reflect the suitability of the technology for treating hypertension.Compared with the Symplicity HTN-3 study, this study used a microtube-irrigated ablation catheter and we chose the main renal artery plus branch method for RDN.It showed that compared with before treatment,the office blood pressure and 24-hour ambulatory blood pressure were significantly lower than the preoperative blood pressure in both groups.Main renal artery plus branch ablation showed the advantage of controlling blood pressure during the 3- 12-month follow-up, but on longer-term follow up, this advantage disappeared.
Currently, main renal artery ablation is the most popular method for RDN.In our study, the main renal artery plus branch ablation group had more ablation points than the main renal artery ablation group.The blood pressure in the main renal artery plus branch ablation group was significantly lower than in the main renal artery ablation group during the 3- 12-month follow-up, and the decrease in mean systolic blood pressure was significantly different (P < 0.05).Animal experiments showed that norepinephrine decreased more in main renal artery ablation than that in the only branch ablation [19].Therefore, we chose main renal artery plus branch ablation instead of only renal artery branch ablation.However, subgroup analysis of the Global Symplicity Registry clinical trial [20] showed that both renal artery branch ablation and main renal artery plus branch ablation had a more pronounced antihypertensive effect on both office blood pressure and ambulatory blood pressure than only main renal artery ablation.Therefore, the appropriate interventional approach may be key to determining the antihypertensive effect of RDN.A clinical study also found results similar to those of our study.Fengler et al.[21] compared 25 patients with resistant hypertension who had main renal artery plus branch ablation and patients who had main renal artery ablation only.Main renal artery plus branch ablation has additional ablation points, which is more conducive to sympathetic blockade.Our findings also suggest that main renal artery plus branch ablation impedance is higher than main renal artery ablation impedance, which may be related to the small branch diameter of the blood vessels.The results showed that both groups had no difference in blood pressure levels at the baseline, but at 3- 12 months,the main renal artery plus branch ablation group had a blood pressure drop more pronounced than that of the main renal artery ablation group.In this study,more patients were observed and followed up for longer.We found the difference in blood pressure between the two groups disappeared and the blood pressure of both groups increased as the follow-up time increased.This phenomenon was not mentioned in previous studies.Because we observed patients for longer than other studies, there was no significant difference in blood pressure between the two groups during long-term follow-up.This phenomenon needs further investigation for confirmation.We speculate that this may be related to the recovery of feedback from the nervous system.
Restrictions and Deficiencies
This was a long-term follow-up, prospective, randomized controlled study of main renal artery ablation and main renal artery plus branch ablation.The small sample size and the single center in this study may have biased the results.Results from a larger randomized controlled study are necessary to show that RDN intervention may be a valuable option for the treatment of resistant hypertension.
Conclusions
The results of this study show that main renal artery plus branch ablation is a safe interventional method,but there was no obvious advantage on long-term follow-up compared with only main renal artery ablation.
Acknowledgments
Support for this study was provided by The Overseas Program of Shanghai University of Chinese Medicine, the Shanghai Key Medical Specialties Construction Project (ZK2019A11), the Shanghai Health and Family Planning Commission Medical Clinical Special Project (201840247),the Young Elite Scientists Sponsorship Program of CAST (QNRC2-B03), the Clinical Advantage Discipline of Health System of Putuo District in Shanghai (2019ysxk01), the Shanghai Traditional Chinese Medicine Inheritance and Technological Innovation Project (ZYCC2019026), and the“ Scientific and Technological Innovation Action Plan” medical innovation research project(20Y11910100).
Conflicts of Interest
The authors declare that they have no competing interests.
 Cardiovascular Innovations and Applications2021年4期
Cardiovascular Innovations and Applications2021年4期
- Cardiovascular Innovations and Applications的其它文章
- Barriers to the Implementation of Primary PCI in the Management of STEMI in Egypt
- Comparison of a 5 F Microtube-Irrigated Ablation Catheter and a General Ablation Catheter in the Treatment of Resistant Hypertension with Renal Denervation
- Clinical Significance of Angiographically Detectable Neovascularity in Patients with Cardiac Myxoma
- ST-Segment Depression in Leads I and aVL:Artifactual or Pathophysiological Findings?
- A Case Report of Radiofrequency Ablation of Typical Atrial Flutter Combined with Atrial Tachycardia