
Knowledge,attitude,and practices related to medication errors among nursing professionals: a questionnaire-based study in a tertiary care hospital
2023-12-15 04:08VishlRjBbuRekhPriydrshini
Frontiers of Nursing 2023年4期
Vishl Rj,L.N.Bbu,Rekh Priydrshini
a Department of Pharmacology, Indira Gandhi Medical College and Research Institute (IGMC &RI), Puducherry 605009, India
bDepartment of Pharmacology, All India Institute of Medical Sciences (AIIMS) Bibinagar, Hyderabad, Telangana 508126, India
Abstract: Objective:To evaluate the level of understanding (knowledge),beliefs (attitude),and behavior (practice) of staff nurses toward medication errors (MEs).Methods:Self-administered questionnaires were distributed to nursing professionals who had at least 1 year of work experience.Each questionnaire contained 19 items assessing “knowledge,” “attitude,” and “practice” attributes toward MEs.Results:Responses from 47 nursing respondents were included for the final analysis.The mean knowledge score was 3.8 ± 1.1 (out of 6);66% and 79% of the respondents had awareness of medication reporting systems and interventions in preventing MEs,respectively.Lack of adequate knowledge in recognizing MEs (P=0.003),or presuming MEs are not as important enough to be reported (P=0.002),was considered as the major reason for under-reporting of MEs.Nurses with higher knowledge score were against administration of medication through a different route than that prescribed by the physician (P=0.023),and tried to rectify an ME (P=0.020) and stayed with the patient until an oral medication had been swallowed (P=0.037).Conclusions:The nursing professionals were aware of the ME reporting system and methods to prevent the occurrence of MEs.They also exhibited a positive attitude and followed optimal practices in controlling MEs.
Keywords: administration errors ? dispensing errors ? medication errors ? nurses ? transcription errors
1.Introduction
Medication error (ME) is an error of commission or omission occurring at any step along the pathway that begins when a clinician prescribes a medication and ends when the patient actually receives the medication.1All MEs are a common form of preventable medical errors and may or may not produce harm.According to the National Coordinating Council for Medication Error Reporting and Prevention (NCC-MERP),MEs are “the preventable events that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the healthcare professional,patient,or consumer.” All the MEs are not adverse drug events (ADE)and vice versa.The preventable harm caused by an ME is considered to be a preventable ADE due to ME.2
MEs are broadly categorized as No Error;Error,No Harm;Error,Harm;Error,Death;which is according to the NCC-MERP.The incidence of MEs appears to be low,but is in the rising trend.
Medical errors are not only monetarily costly,but also costly in terms of loss of trust in the healthcare system by patients,reduced patient satisfaction,and a degraded morale among healthcare professionals,who often feel helpless about the situation.The majority of medical errors occur not as a result of incompetence or recklessness on the part of nurses and other healthcare workers,but rather as a result of faulty systems,including fragmented processes and working conditions (e.g.,nurses exhausted from working double shifts).
The report published by the Institute of Medicine in 1999 declared that the total number of deaths occurred as a result of medical mistakes was between 44,000 and 98,000.Globally,the incidence and prevalence of MEs are increasing and leading to wastage of healthcare expenditure;almost 1% of the total global health expenditure is associated with ME.3Approximately 10% of all hospitalizations are drug-related,and around half of these hospitalizations are due to preventable ADEs.4MEs account for around one death every day and approximately 1.3 million people getting injured in the United States.Despite incomplete data,similar rates of MEs are estimated in the low-and middle-income countries and the impact is about twice as much in terms of the number of years of healthy life lost.A global initiative was launched by the World Health Organization (WHO) on March 2017,expecting a 50% reduction in severe,avoidable medicationassociated harm in all countries over the next 5 years.This is WHO’s third global patient safety challenge.3
MEs can occur at any step in the pathway of the medication process (prescribing [ordering],transcription,dispensing,administration,and monitoring) in which medical personnel are involved.Errors in the administration step (i.e.,giving medicine to patients),the crucial step in the medication process,contribute to around 87% of MEs.5As nurses directly handle the drug administration to patients,they play a vital role in patient care and patient’s quality of life.MEs occur more commonly among nurses than in other healthcare professionals.6The transition of patients between wards,shortage of staff,misinterpretation of verbal orders,ignorance in taking allergy history,deficit in pharmacological knowledge and mathematical skills,poor practical skills,and accidental occurrence are showcased to be some of the reasons for ME by nurses.7–12Understanding the fundamental issues associated with administering medications in a hospital setting is key to prevent these errors.
Safety of the patient is one of the main responsibilities of the medical care professional,including nurses.The essential step in preventing MEs (in particular administration errors) is a proper understanding of the prevalence and factors responsible for MEs and reporting systems of MEs among nursing professional.This will help health policymakers to propose and implement effective interventions to reduce the negative impact of MEs on the healthcare system.Hence,this study was planned to evaluate the level of understanding (knowledge),beliefs (attitude),and behavior (practice) of staff nurses toward MEs.
2.Methods
2.1.Study design,setting,and subjects
This cross-sectional observational study (Questionnairebased study) was conducted among nursing professionals in a tertiary care teaching institute of Puducherry.Consenting and eligible nurses were enrolled in the study for a period of 6 months.Nurses registered with the Indian Nursing Council or other affiliate State Councils and who had at least 1 year of work experience after graduation were included.Nurses with Auxiliary Nursing&Midwifery (ANMs) degrees were excluded.
2.2.Sample size
The minimum recommended sample size for the survey was calculated as 60 nurses with a margin of error of 10% and confidence level of 95%.The sample size was estimated based on the available finite population size of 151 and with a response distribution of 50%.Convenience sampling technique was adopted.
2.3.Study procedure
The study was initiated after obtaining scientific and ethical approval from the Institute.Written informed consent were obtained from the eligible nurses.All the nurses were asked to fill in a self-administered questionnaire after briefing about the study.The distributed self-administered questionnaire contained information pertaining to their knowledge,attitudes,and practice with regard to MEs.The necessary instructions about filling the questionnaire were elaborated to all the respondents.
The questionnaire was anonymous and included demographic details;it had 19 items under three sections,6 items under the “knowledge” section,6 items under the “attitude” section,and 7 items under the “practice” section.The “knowledge” section was composed of partially categorized questions as well as a single closed-ended question;the “attitude” section included Likert scale-type questions,and the “practice” section contained only closed-ended questions.
The content validity of the questionnaire was evaluated through Content Validity Index (CVI) of the individual items.An expert panel of four faculty members (with expertise and experience in MEs) was constituted.A 4-point Likert scale (1=not relevant,2=somewhat relevant,3=relevant,4=very relevant) was utilized and each expert had independently rated the relevance.A particular questionnaire-item was considered relevant if the ratings ascribed were “3” and “4”;and together these rating-points were considered as a“favorable” response to the item;similarly,ratings “1”and “2” were together considered as an “unfavorable”response to the item and the questionnaire-item was considered irrelevant.All the 19 questionnaire items were retained,as the CVI of each item was above the prefixed cut-offs (75%).
2.4.Statistical analysis
Analysis of data was performed both manually and by means of computerized programs.Data were represented in frequencies and percentages.Descriptive statistics was performed to analyze the data.The data were recorded and analyzed using Microsoft Excel and GraphPad InStat.Item analysis was also done to estimate item statistics,inter-item correlation,item-total statistics,and scale statistics in SPSS (IBM Corporation,Armonk,New York,United States) (under reliability statistics).Data were expressed as mean ± standard deviation (SD) for continuous variables and percentages (%)for categorical variables.Two-tailedPvalues were used and aPvalue less than 0.05 (P<0.05) was considered as statistically significant.
3.Results
The questionnaires were distributed to 63 nursing professionals,out of which 54 responded.Seven responses were excluded due to incomplete data.Hence,responses from 47 respondents were included for the final analysis.The majority of nursing care respondents were from the age group of 31-35 years(55%) followed by 26-30 years (34%).The educational qualification of the respondents was B.Sc.Nursing,30(64%) followed by M.Sc.Nursing,10 (21%) of which the majority were working with the designation of Nursing Officers,33 (70%).The majority of the respondents (30,64%) were in the experience bracket of 6–10 years.The respondents who took part in the study were those predominantly posted in the Male Medical Ward 15 (32%)followed by the Pediatric Ward 8 (17%).The duration of the work varied from <2 h to >5 h,of which the majority were working for <2 h (43%) (Table 1).

Table 1.Baseline demographic characteristics (N=47).
Only 36% of the respondents were aware of the precise definition of ME.Likewise,43% and 60% of the participants were aware of the computerized prescriber order entry (CPOE) systems and Iook-alike and sound-alike (LASA)/sound-alike and look-alike (SALA)medications,respectively.On the contrary,66% and 79% of the nurses had awareness of ME reporting systems and interventions in preventing MEs,respectively.The mean knowledge score was 3.8 ± 1.1 (out of 6) among the respondents.The demographic characteristics were not found to influence the knowledge score achieved (P>0.05) (Table 2).Neither lack of knowledge in identifying MEs (P=0.003) nor considering MEs as not important enough to be reported (P=0.002) was asserted as the major barriers for reporting of MEs(P<0.05,chi-square goodness-of-fit tests) (Figure 1).

Figure 1.Attitude on barriers of MEs.

Table 2.Baseline demographic characteristics categorized based on the knowledge score (N=47).
Among those with a better knowledge score(>3),97%,85%,and 82% of the nurses were against administration of medication through a different route than that prescribed by the physician (P=0.023),tried to rectify an ME (P=0.020),and stayed with the patient until an oral medication had been swallowed (P=0.037),respectively (Table 3).
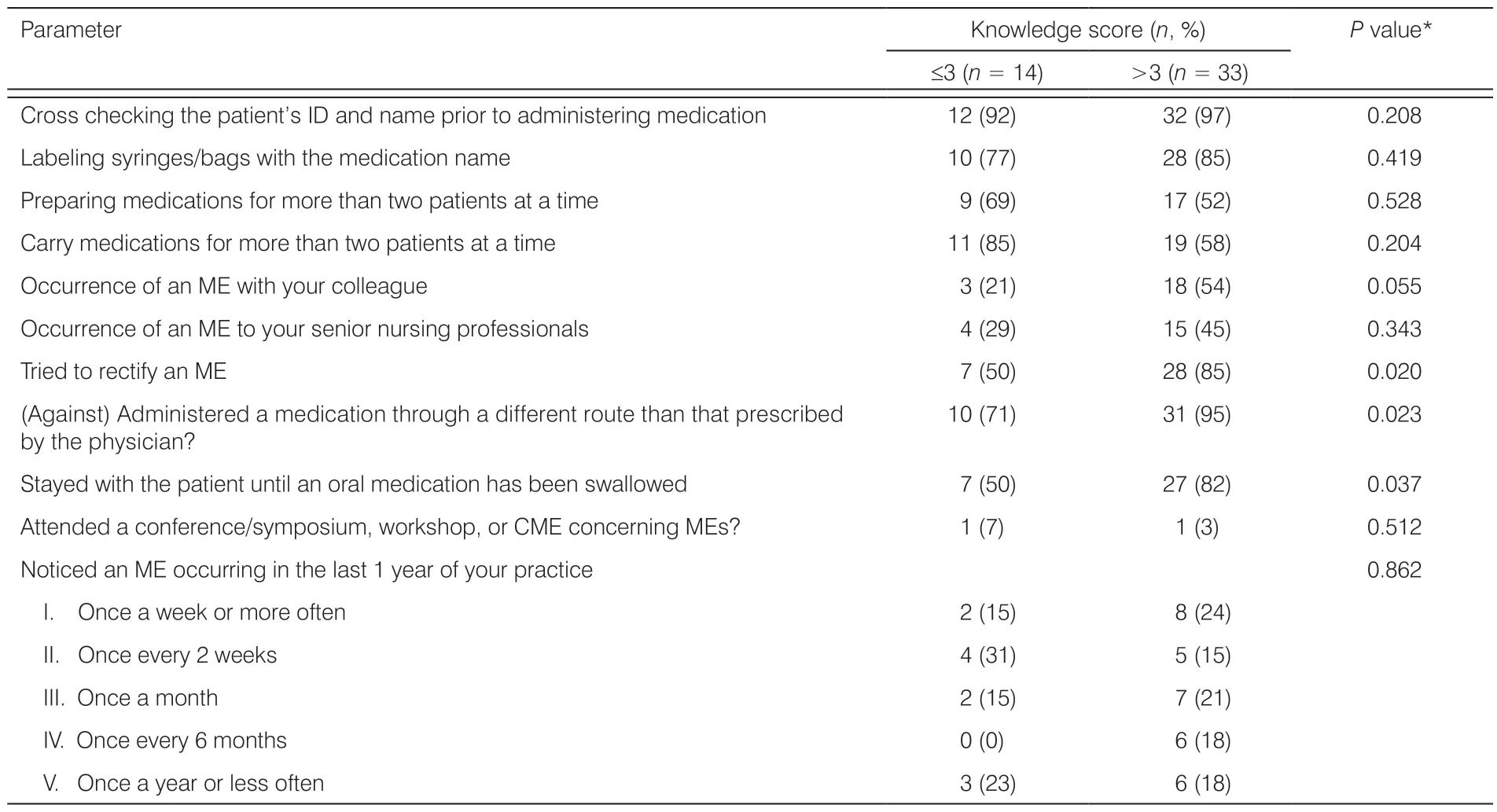
Table 3.Practice parameters based on the knowledge score (N=47).
The results strongly reaffirmed the necessity for an independent institutional body for reporting ME(P<0.001) and a compulsory refreshment program on medical error (P<0.001).Neither usage of multiple medications (P=0.027) nor accurate flow rate maintenance of IV fluids (P=0.034) was considered as reasons for occurrence of MEs (Figure 2).
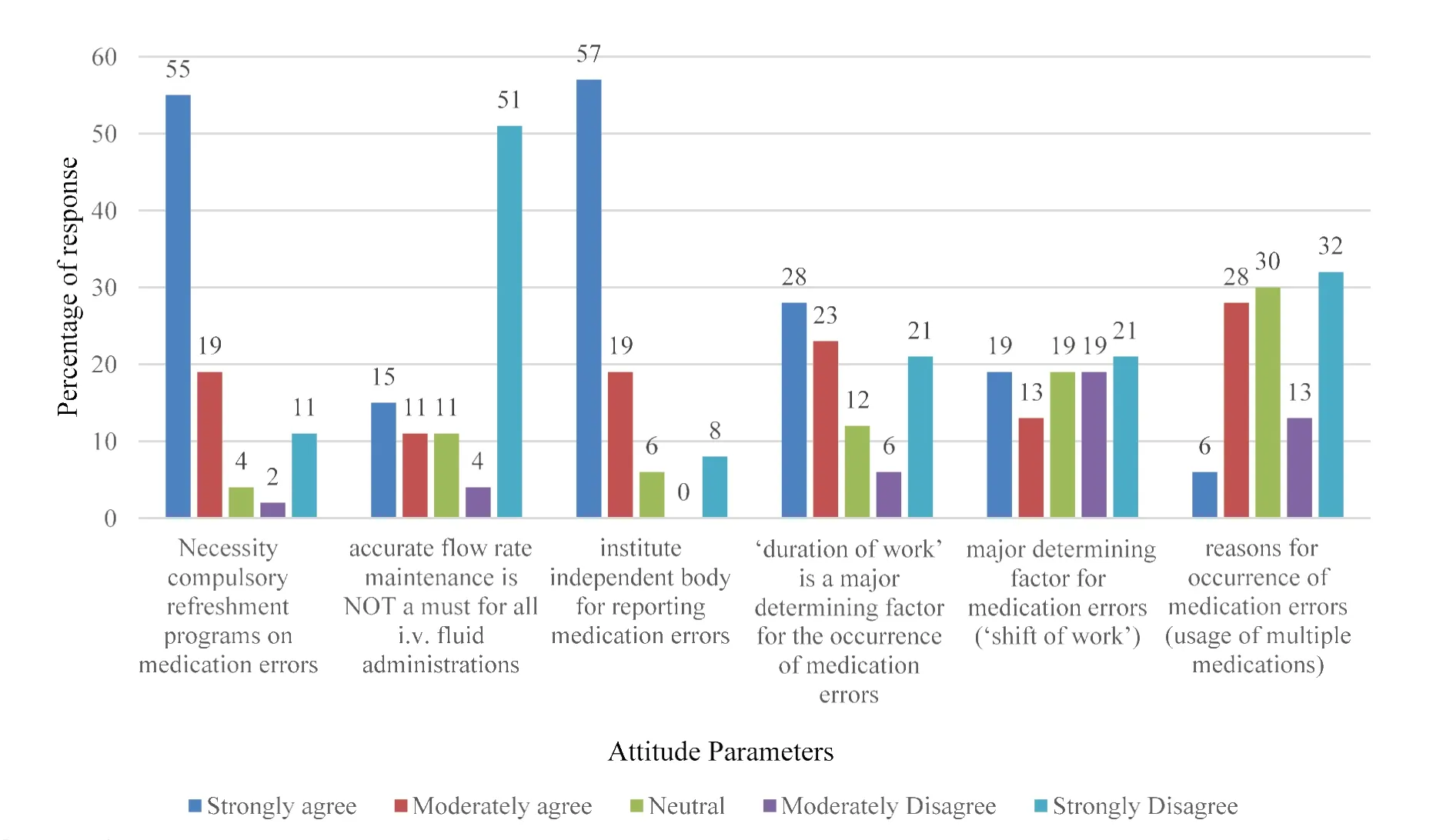
Figure 2.Attitude parameters.
4.Discussion
Our study to assess the knowledge,attitude,and practice on MEs among the nursing staff has drawn responses from nursing staff with educational qualifications mostly from B.Sc.and M.Sc.Nursing backgrounds.The years of experience for most of them were between 6 and 10 years (64%).Most of them were Nursing Officers,and the remaining were Staff Nurses.The demographic characteristics including age,educational qualification,designation,years of experience,place of work,and duration of work were not found to be major determinants of knowledge of ME.
I shall keep my word, said the prince; but may a little water be taken to the roof so that I may make my last ablution? To this request the king consented
Among the barriers for under-reporting of MEs in our study,none of the responses substantiate significantly to portray that any such barriers do really have an impact on under-reporting of MEs.Although some respondents felt that forgetting to report and lack of knowledge of how to report could be a barrier,they could not be relied upon as promoters of MEs,as they did not yield statistical significance.Moreover,a significant number of respondents strongly disagreed that lack of knowledge among them in identifying MEs could contribute as a barrier to report ME.These findings very well indicate that lack of knowledge on reporting ME is largely unlikely to be a causative factor for ME.The typical reasons for under-reporting of MEs or barriers seen in various other studies were the fear of consequences,fear of losing job,fear of reaction from senior officials,fear of negative feedback from patients,and the fear of disciplinary action against them.13–18Only 13% of our study participants opined fear as a barrier to reporting ME,while 11% felt that the adverse consequences of reporting could be a barrier.The above is one of the major contrasting findings of our study population when compared with other studies.
Furthermore,the nursing faculty would have thought that giving a negative response (that the barrier to reporting ME is due to fear of consequences or liability,and others) would be an insult to their reputation.This outlook would have made our study participants(nurses) judgmental in giving a negative response,like the one mentioned above.This approach could be due to the fear of being judged in a negative way,which in fact would be a backlash to their performance,quality of work,16or a stigma15at the workplace.Studies conducted by Lin and Ma19reinforce this fact in an indirect way,wherein nurses were willing to report MEs if there were no adverse consequences after reporting them.The above study also shows that the nursing faculties were very conscious of maintaining their reputation at the workplace.
Although other studies have shown detailed paperwork,lack of time,lack of awareness of reporting processes,forgetting to report during busy hours,and lack of awareness of the importance of reporting as the other barriers for reporting,yet our study participants were not convinced that these could be contributing factors as barriers for reporting MEs.
Also,a significant number of respondents felt that reporting an ME is important and it also translated in their practice wherein those with a higher knowledge score tried to rectify an ME and have never administered a medication through a different route than that prescribed by a physician,and even stayed with a patient until an oral medication had been swallowed.
Another major finding in our study is that only 4%of the study populations had attended a symposium or CME concerning MEs.This is well substantiated in our study,as a significant proportion of them felt that a compulsory refreshment program on ME-reporting is necessary.This attitude among the nursing fraternity is reasonable and heartening,because studies conducted by Tshiamo et al.8and Di Simone et al.20had documented the fact that preserving,strengthening nursing education,and reinforcing pharmacological knowledge and skills of drug administration as training methods would prevent MEs among the nursing population.
A significant number of the study participants had opined on instituting an independent body for reporting MEs.Whereas a lack of tutorships in the way of CME,refreshment,or training program could be a reason for their opinion on instituting an independent body for reporting MEs,yet,long working hours,heavy patient load,less staff,and preoccupation on safety practices while using multiple medications could have obviated their focus on reporting MEs,and hence they would have felt the necessity of an independent body for reporting the same.
Although other systems like chart reviews,audit activities,21and web-based reporting systems22are in place for reporting MEs elsewhere,whether the nursing faculty in our setup can follow these activities is highly questionable.Lack of manpower,paucity of fundings,deficiency in training,or administrative constraints could be some of the reasons at our Institute.
5.Conclusions
In our study,the study population had adequate knowledge of ME practices,they understood the importance of safe medication practices,and also inculcated them in their profession.They emphasized that lack of knowledge could not be a barrier for reporting MEs,and yet,many felt a necessity for refreshment programs on MEs.
Although a majority of the nurses were not able to identify the precise definition of ME,they were aware of the reporting system for MEs,ways to prevent them,portrayed a positive attitude,and followed optimal practices in controlling MEs.
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.The study was approved by the Institute Ethics Committee of IGMC &RI (Project Proposal Number: 32/213/IEC-25/PP/2019).
Conflicts of interest
All contributing authors declare no conflicts of interest.
- Frontiers of Nursing的其它文章
- Impacts of fighting against COVID-19 on critical care nurses’ psychological and physical health: a literature review
- Investigating adverse events in long-term care facilities: a systematized review
- A bibliometric analysis and visualization of research on heart failure complicated with malnutrition
- Implementation and achievements of enhanced recovery after surgery program in perioperative management of gastric cancer patients?
- Dietary adherence and the associated factors among Indonesian patients with type 2 diabetes: what should we be concerned about??
- Factors related to self-management behavior among persons with mildto-moderate chronic obstructive pulmonary disease in Wenzhou,China