
Predictors of hemorrhagic manifestations in dengue: A prospective observational study from the Hadoti region of Rajasthan
2023-12-16 09:14ShivCharanJeliaDevendraAjmeraDivyaAiranRanjeetBairwaYogeshMeena
Journal of Acute Disease 2023年6期
Shiv Charan Jelia, Devendra Ajmera, Divya Airan, Ranjeet Bairwa, Yogesh Meena
Department of General Medicine, Government Medical College, Kota, Rajasthan, India
ABSTRACT
KEYWORDS: Dengue fever; Dengue hemorrhagic fever; Complicated dengue; Bleeding
1.Introduction
Dengue fever is one of the most rapidly spreading arboviral diseases in the world.An estimated 3.9 billion people are at risk for dengue virus (DENV) infection with around 100 to 400 million estimated cases per year[1].According to the estimation of the World Health Organization, the incidence of DENV infection has increased drastically in the recent years, with an over 19-fold increase in reported cases within two decades, from half a million in 2000 to 5.2 million in 2019[1].As per data provided by the Director General of Health Services, in 2022, India recorded around 233 251 cases which is more than two times the cases reported in 2018 (101 192 cases)[2].The vector for dengue is the Aedes aegypti mosquito which is widely distributed across tropical and subtropical areas.Based on the antigenic difference, dengue fever can be divided into four serotypes: DENV 1 to DENV 4[2].Most of the DENV-infected people are asymptomatic or have only mild symptoms such as fever and myalgia.Some patients may develop severe illness resulting in hemorrhagic manifestations and shock which can become lifethreatening[3].The clinical course of the disease is divided into febrile, critical, and recovery phases.The incubation period is mostly about 4 to 7 days.The acute febrile phase has mild symptoms such as headache, myalgia, weakness, joint pains, vomiting, and abdominal pain[1-4].As per clinical manifestations, DENV infection can be classified into 3 categories: dengue fever, dengue hemorrhagic fever, and dengue shock syndrome[5].The clinical picture of dengue fever is demonstrated by thrombocytopenia, raised hemoglobin and hematocrit, and leucopenia[6].Several factors, such as secondary infections, thrombocytopenia, comorbidities, extremes of age, and bleeding manifestations, have been identified to influence disease progression and can lead to severe dengue[7].
There are no clear and well-understood mechanisms responsible for hemorrhagic manifestations in dengue.Hemorrhage in dengue may be attributed to various mechanisms such as thrombocytopenia,endothelium defect, and platelet dysfunction[8].Coagulation dysfunction can also be responsible for bleeding in dengue patients.A few research have shown significant coagulopathy in dengue[8,9].Bleeding manifestations increase mortality and morbidity in dengue patients which is why timely detection and management of bleeding manifestations is necessary to reduce further complications in dengue patients.This study aims to identify predictors of hemorrhagic manifestations in dengue patients.With early identification of high-risk patients, mortality and morbidity due to infection can be reduced.
2.Patients and methods
2.1.Study setting and design
This is a prospective observational study.It was conducted in the Department of General Medicine, Government Medical College,Kota, and the Group of associated hospitals, Kota, from May to October, 2023.
2.2.Ethical approval
Ethical clearance was taken from the Institutional Ethical Committee of Medical College.All the patients were explained in detail about this study and written informed consent in their native language was obtained for each patient before their enrollment in the study.
2.3.Inclusion and exclusion criteria
200 Patients admitted with acute febrile illness who were diagnosed with dengue (seropositive for dengue NS1 antigen and/or IgM antibody) were included in this study.
Patients with a history of pre-existing bleeding disorders, on anticoagulant or antiplatelet therapy, pregnant and menstruating women, and women on hormonal contraceptives were excluded from the study.Patients with chronic diseases that can affect the coagulation profile such as chronic kidney disease, neoplasms, and autoimmune diseases were also excluded from the study.
2.4.Methodology
All the patients with DENV infection were investigated for various biochemical parameters such as complete blood count, renal function tests, liver function tests, coagulation profiles, and lipid profiles.A detailed history was taken and a clinical examination was done.If required, necessary imaging was done.All the patients were followed till the end point like recovery or death.
The following symptoms were considered as bleeding manifestations:purpura, ecchymoses, or petechiae; bleeding from the gastrointestinal tract, injection sites, mucosa, or other sites; intracranial bleeding;tourniquet test is positive; melena or hematemesis.
2.5.Primary and secondary outcomes
The primary outcomes included the bleeding manifestations and duration of hospital stay.The secondary outcome included mortality or recovery.
2.6.Statistical analysis
Excel 2017 and IBM SPSS Statistics version 29.0 were used.Categorical variables were expressed as numbers and percentages.Continuous variables were expressed as mean with standard deviation.They were analyzed by Chi-square test, Mann-Whitney U test and unpaired t-test.P value less than 0.05 was considered significant.
3.Results
A total of 689 patients were admitted to the medicine ward and intensive care unit with acute febrile illness.Out of these 689 patients, 270 were seropositive for DENV infection.38 Patients were excluded based on exclusion criteria and 32 patients refused to participate.The final study size was 200 patients who were seropositive for DENV infection, fulfilling inclusion criteria and giving consent for the study (Figure 1).

Figure 1.The study flowchart.
3.1.Demographic and clinical characteristics
The majority of patients in our study were under the age of 30, with a mean age of (28.6±14.0) years.The male-female ratio was around 2?1.Student was the majority occupation followed by housewife.The most common presenting symptom was fever followed by myalgia,nausea, and vomiting.Hepatomegaly and splenomegaly were presented in 21 (10.5%) and 42 (21.0%) patients, respectively.Third spacing in the form of ascites and pleural effusion was present in 40(20.0%) and 31 (15.5) patients, respectively.Around one-fourth of the patients had hemorrhagic manifestations during illness (Table 1).
3.2.Laboratory profile
Mean values of various parameters are shown in Table 2 comparing patients with and without hemorrhagic manifestations.Mean age showed a statistically significant correlation with bleeding manifestations (P=0.032).Hemoglobin level and hematocrit values did not show a significant correlation with hemorrhagic manifestations.There was an increased white blood cell count,and absolute neutrophil count in patients with bleeding (P<0.001),but there was no correlation of monocyte and lymphocyte counts with bleeding symptoms.The decreased number of platelets was significant for bleeding (P=0.003).The neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) also showed astatistically significant correlation with hemorrhagic manifestations(P<0.001).Platelet indices viz mean platelet volume (P<0.001)and platelet distribution width (P=0.031) also showed a significant correlation with bleeding.Renal function tests such as blood urea and creatinine values did not statistically differ in two the groups.Liver function tests viz total bilirubin, serum glutamic-oxaloacetic transaminase (SGOT), serum glutamic pyruvic transaminase (SGPT), and serum albumin, all had statistically significant correlation with bleeding manifestations(P<0.001).The lipid profile did not have any correlation with bleeding in dengue patients.
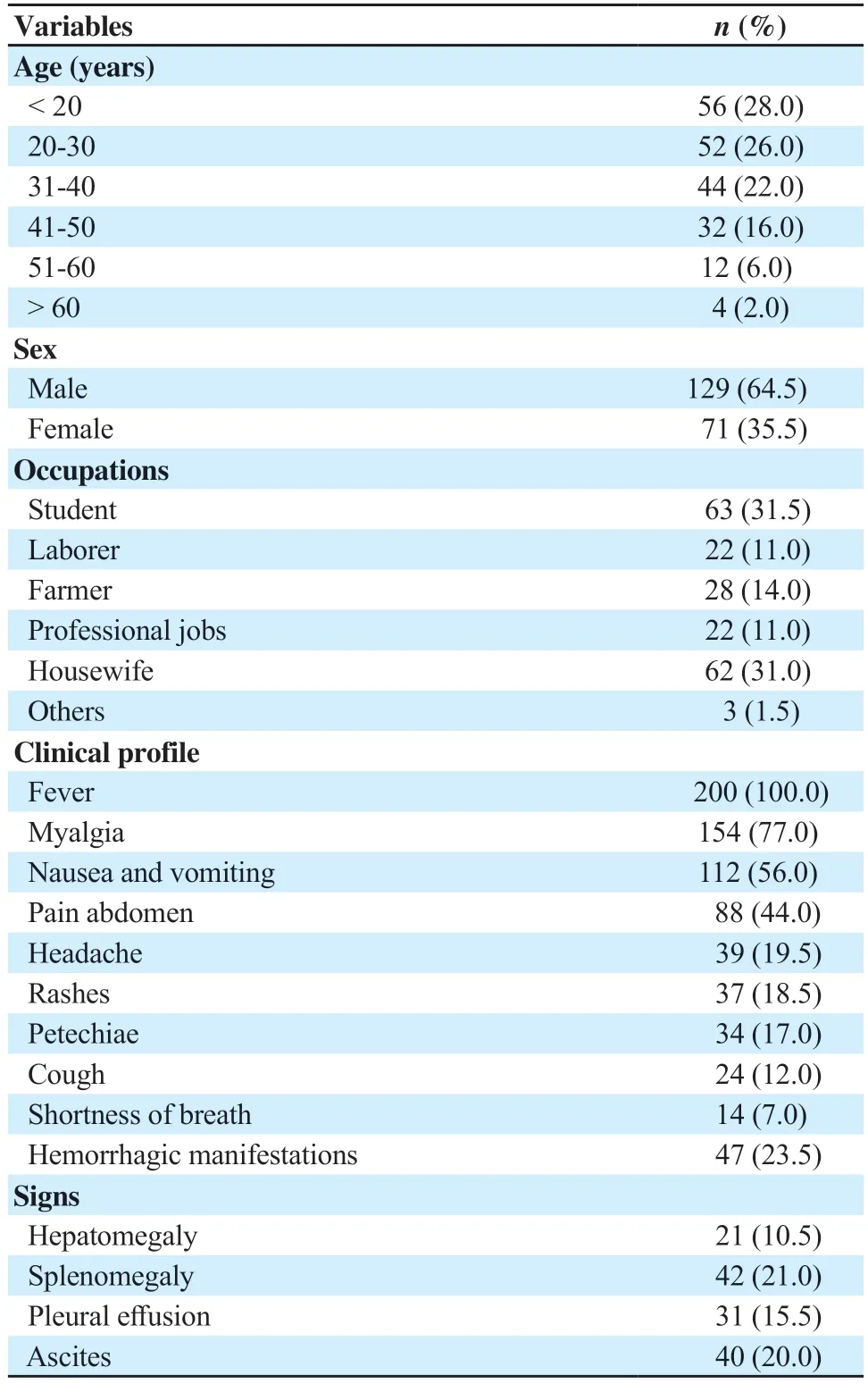
Table 1.Demographic and clinical characteristics (n=200).
Although all coagulation parameters were deranged in patients with DENV infection, we did not find a significant correlation with bleeding with prothrombin time (PT), international normalized ratio(INR), and activated partial thromboplastin time (APTT) except for D-dimer.Raised D-dimer levels were associated with hemorrhagic manifestations (P<0.001).
In terms of outcome, bleeding in dengue patients was associated with increased duration of hospital stay and increased mortality(P<0.001).

Table 2.Comparison of laboratory profile between patients with and without bleeding (n=200).

Table 3.Comparison of clinical signs between patients with and without bleeding (n=200).
3.3.Clinical findings
Hepatomegaly and splenomegaly were not correlated with an increased incidence of bleeding.However pleural effusion and ascites were significantly associated with bleeding manifestations(P<0.001) (Table 3).
4.Discussion
Hemorrhagic manifestations in dengue fever are due to increased vascular permeability leading to plasma leakage and abnormal hemostasis.Bleeding in DENV infection can range from petechiae,purpura, hematoma, gum bleeding, epistaxis, and subconjunctival hemorrhage to life-threatening bleeding manifestations such as gastrointestinal bleeding and intracranial bleeding[5].
In our study, around one-fourth of total patients (23.5%) had hemorrhagic manifestations.This result is similar to a study conducted by Hamsa et al.[10] which had 28.1% of patients with bleeding manifestations.Few other studies also found similar results with bleeding in 25%-30% of patients[11,12].Another study by Kulasinghe et al.had a lower incidence (8.2%) of hemorrhagic manifestations[9].This variation in bleeding incidence could be due to different admission guidelines by different hospitals.
The present study did not find any statistically significant correlation between hemoglobin level and hematocrit with bleeding manifestations.This is supported by studies by Diaz-Quijano et al.and Patel et al.[13,14], which did not correlate hemoglobin level and hematocrit level with bleeding.We found leukocytosis and neutrophilia significantly associated with hemorrhagic manifestations.This is similar to a study by Diaz-Quijano et al.[13].However, a study by Patel et al.[14] did not find a correlation between bleeding and leukocytosis.There was no association between lymphocyte counts and monocyte count with bleeding manifestations.We found a significant association between thrombocytopenia and bleeding.Kadadavar et al.[15] in their study also found a significant correlation between thrombocytopenia and bleeding.There are a few other studies also supporting this correlation[10,13,14,16].There was a significant association between bleeding manifestations with NLR and PLR.Koundinya et al.[17]also found similar results with NLR as a hemorrhagic predictor.We did not find a study showing PLR comparison in dengue patients.
In the present study, blood urea and creatinine did not have any significant correlation with bleeding manifestations.A study by Patel et al.[14] also had similar results.Few other studies also did not find any correlation between bleeding in dengue with renal function tests[18-20].All parameters of liver function tests had a statistically significant association with bleeding manifestations.In our study, raised values of total bilirubin, SGOT, and SGPT were associated with increased incidence of bleeding in dengue patients meanwhile lower values of serum albumin were associated with bleeding.Previous studies differ slightly in different parameters.Patel et al.[14] in a study found a significant association of bleeding manifestations with raised SGPT, SGOT, and decreased albumin levels but there was no correlation with bilirubin levels.Waheed et al.[19] showed an increased incidence of bleeding manifestations in patients with raised levels of SGPT and did not find an association with bilirubin and albumin levels.Hassan et al.[18] did not find an association of bleeding incidence with any liver function test parameter.Chamnanchanunt et al.[20] showed an association with raised SGOT values but not with SGPT levels.Shivbalan et al.[16] in their study found a positive correlation between raised SGPT levels and hemorrhagic manifestations.Wang et al.[21] found an association between decreased levels of albumin with complicated dengue.
The exact pathophysiology behind coagulation dysfunction in dengue fever is not known.There are theories regarding various mechanisms.The PT is indicative of the extrinsic pathway of coagulation and activated partial thromboplastin time is an indicator of the intrinsic pathway of the coagulation system.In DENV infection, prolongation of PT and APTT is seen.It may be due to the downregulation of the synthesis of specific coagulation factors or an increase in the consumption of coagulation factors.The non-structural protein 1 of the DENV can inhibit prothrombin activation by binding to prothrombin.Prolongation in APTT can be explainedby this mechanism[22].Hassan et al.[18] stated that there can be a reduction of certain specific coagulation factors such as factor 2,5,7,8,9,10, anti-thrombin, and alpha 2 antiplasmin which results in coagulation abnormalities and bleeding manifestations.In the present study, we did not find a significant association between PT, INR, and APTT with bleeding manifestations, however there was a signification association of bleeding with raised levels of D-dimer.The exact mechanisms for raised levels of D-dimer have not been known, but few studies suggested that coagulopathy due to disseminated intravascular coagulation is responsible for increased D-dimer levels[14].Similarly, Hassan et al.[18] did not find an association between bleeding with APTT but they also did not find an association with raised D-dimer level.A study by Diaz-Quijano et al.[13] also supported our results by showing no association of PT with bleeding.Sharif et al.[23] in their study did not correlate bleeding with PT but with prolonged APTT.Patel et al.[14] showed a correlation between hemorrhagic manifestations with raised PT,INR, APTT, and D-dimer levels.
Hepatic involvement in DENV infection is common in the form of microvesicular fatty changes, hepatocyte necrosis, Kupffer cells hyperplasia and destruction, Councilman Bodies, and portal tract infiltrates.This liver involvement leads to hyperbilirubinemia and transaminitis[24].In our study, 10.5% of patients had hepatomegaly and 21.0% of patients had splenomegaly.On comparing clinical findings in bleeding and non-bleeding groups, we did not find a statistically significant association of hepato-splenomegaly with hemorrhagic manifestations.Plasma leakage in DENV infection leads to gall bladder wall edema, pleural effusion, and ascites.On statistical analysis, we found that patients with ascites and pleural effusion had an increased incidence of bleeding.Shivbalan et al.[16]and Ikram et al.[19] in their studies also demonstrated a positive correlation between ascites and pleural effusion with hemorrhagic manifestations in DENV infection.
In this study which included 200 patients with DENV infection,47 patients showed bleeding manifestations during the disease.Leukocytosis, neutrophilia, andthrombocytopenia can be used as hematological predictors of bleeding in DENV infection.Hyperbilirubinemia, transaminitis, decreased serum albumins,and raised D-dimer can also serve as biochemical and coagulation predictors of hemorrhage manifestations in DENV infection.Bleeding in DENV infection can be life-threatening and we aim to identify complications early and manage accordingly.These laboratory and clinical parameters can be useful in predicting hemorrhagic manifestations and identifying high-risk patients.
Conflict of interest statement
The authors report no conflict of interest.
Funding
This study received no extramural funding.
Data availability statement
The data supporting the findings of this study are available from the corresponding authors upon request.
Authors' contributions
SCJ formulated the study concept and developed the study design.D Ajmera did a literature search.Data collection was done by D Airan, RB and YM.RB and YM did data and statistical analysis.Manuscript preparation was done by D Ajmera and D Airan.All authors have reviewed and approved the final version of the manuscript.
 Journal of Acute Disease2023年6期
Journal of Acute Disease2023年6期
- Journal of Acute Disease的其它文章
- Clinical profile of medication-related emergencies among patients presenting to the emergency department: An observational study
- Risk factors for development of pneumothorax in patients with COVID-19 at a government health facility in North India: An exploratory case-control study
- Neurological manifestations of COVID-19 infection: A case series
- Imipenem/cilastatin-induced acute eosinophilic pneumonia: A case report
- A public health perspective on dengue in Bangladesh in the twenty-first century
- COVID-19 mortality trends before and after the national vaccination program in Iran: A joinpoint regression analysis