
The feasibility and preliminary efficacy of narrative exposure therapy on post-traumatic stress disorder among Syrian refugees in Jordan
2023-11-26 05:22NdeenSmikLeighAnnSimmonsBynAdulhqLtefAliDrds
Ndeen Smik ,Leigh Ann Simmons ,Byn Adulhq ,Ltef Ali Drds ,*
a School of Nursing, The University of Jordan, Amman, Jordan
b The Betty Irene Moore School of Nursing, UC Davis, Sacramento, CA, USA
c School for International Training, Amman, Jordan
Keywords:Anxiety Depression Jordan Narration Narrative therapy Post-traumatic stress disorder Refugees
ABSTRACT Objective: Post-traumatic stress disorder (PTSD),anxiety,and depression are common mental health disorders among refugees,and all require immediate mental health support to prevent short-and longterm detrimental health outcomes.The purpose of this study was to evaluate the feasibility and preliminary efficacy of narrative exposure therapy (NET) in reducing symptoms of PTSD,depression,and anxiety among Syrian refugees residing in Jordan.Methods: A two-arm randomized control trial was utilized.A total of 40 Syrian refugees aged 18 to 64 diagnosed with PTSD were randomly allocated to either the NET intervention group (n=20) or the waitlist control group (n=20) using a computer-generated allocation list with 1:1 allocation.PTSD symptoms were evaluated using the Arabic rendition of the Harvard Trauma Questionnaire,while depression and anxiety symptoms were appraised using the Arabic adaptation of the Hopkins Symptoms Checklist-25.Descriptive statistics were employed to characterize the sample and survey data.Independent t-tests were conducted to assess mean score differences in PTSD,anxiety,and depression between the intervention and control groups.Results: Post NET intervention,significant reductions in PTSD(t=-10.00,P <0.001),anxiety(t=-9.46,P <0.001),and depression (t=-6.00, P <0.001) scores were observed in the intervention group compared to the control group.Effect sizes were moderate for the trauma (Cohen’s d=0.73) and depression (Cohen’s d=0.79) symptoms and notably large for anxiety symptoms (Cohen’s d=0.97).There were no adverse events related to study participation.The intervention achieved a 100% participant retention rate.Conclusions: The results pertaining to retention rate,adherence to the study protocol,data completeness,cultural congruence,and participants’ satisfaction provided strong support for the future implementation of the full-scale RCT.NET may be a feasible and helpful approach for refugees and other patients with PTSD,anxiety,and depression.
What is known?
· Narrative exposure therapy has been frequently used with refugees suffering from post-traumatic stress disorder,depression,and anxiety.Evidence on the effectiveness of narrative exposure therapy among patients with these disorders is promising but not conclusive.
· There remains a need to expand the current evidence on this therapy in low-resource settings before drawing firm conclusions on its overall beneficial effects.
What is new?
· The study highlights the promising initial effectiveness of narrative exposure therapy in reducing symptoms of posttraumatic stress disorder,depression,and anxiety when compared to no treatment.Notably,all participants attended every narrative exposure therapy session without dropouts,which is unusual among refugees.Immediate symptom reduction post narrative exposure therapy was observed,and more substantial reductions typically occur within three months after treatment.
1.Introduction
Over the past 70 years,90 million refugees from countries all over the world have been registered under the United Nations High Commissioner for Refugees (UNHCR).In 2021 alone,the UNHCR estimated the number of refugees worldwide to be approximately 27 million,in addition to the 4.5 million asylum seekers,and these numbers are only expected to increase given the ongoing wars across several continents,including Eastern Europe,Asia,Africa,and South America[1].The Syrian refugee crisis has been identified as the largest humanitarian and refugee crisis of our time,with the Syrian conflict accounting for recording a high number of forced displacements[2].Data show that by the end of 2021,more than 5 million Syrian refugees were forcibly displaced outside Syria.The vast majority of them(4 million)were displaced to Turkey,Jordan,Lebanon,Iraq,and Egypt[3].
Compared to the general population,refugees are at higher risk of experiencing psychological problems,the most common of which is post-traumatic stress disorder (PTSD).According to the American Psychological Association (APA),PTSD is defined as a disorder caused by exposure to a traumatic event either directly by being exposed to the trauma,indirectly by witnessing the trauma,or by knowing that a family member or close friend was exposed to the traumatic event.It is characterized by intrusive thoughts,flashbacks,alteration in arousal and reactivity,disturbances in sleep,poor concentration,and negative mood fluctuations,all of which lead to significant occupational,social,and interpersonal dysfunction [4].A recent systematic review and meta-analysis [5]showed that the prevalence of PTSD in refugees and asylum seekers was 31.46%(95%CI 24.43%-38.5%).Among Syrian refugees,studies have documented rates ranging from 29.9%in a sample of refugees residing in Turkey and Sweden[6]to 34.9%in a sample residing in Germany [7].
Developing PTSD can have significant negative consequences on mental well-being,physical health,and individual and family functioning [8,9].Refugees may be exposed to other traumatic events as a result of the war or displacement,physical assault,sexual assault/rape,torture,and incarceration.Experiencing one or more of these traumas significantly exacerbates the severity of PTSD and decreases the odds of a healthy recovery[10].Addressing PTSD symptoms among refugees is warranted to prevent potential short-and long-term detrimental health outcomes.Research evidence introduced several interventions,including prolonged exposure(PE)[11],eye movement desensitization and reprocessing(EMDR) [12],trauma-focused cognitive behavioral therapy (TFCBT) [13],psychopharmacology [14],and narrative exposure therapy (NET).The latter,NET,has been found to be a promising approach to reducing symptoms of PTSD for refugees [15-17].
1.1.Narrative exposure therapy (NET)
NET is a short-term,trauma-focused cognitive behavior therapy(TF-CBT) [18].It has been most frequently used in community settings and with individuals who experienced trauma due to political,cultural,or social forces,including refugees [19].NET builds on the theory of emotional processing,which states that understanding the neural network of fear/trauma is essential to developing an effective intervention for PTSD symptoms.According to Schauer,Elbert,and Neuner [18],memories of traumatic events often lack autobiographical information and are dominated by sensory-perceptual ones.As such,putting these anxiety-provoking memories into context helps to rebuild the autobiographical memory,thereby relieving anxiety [18].NET aims to habituate the emotional response and organize the fragmented details related to traumatic events by re-experiencing each painful memory separately within a coherent chronological narrative of events [20].
NET is also directly related to the work on memory functioning.According to Elbert,Schauer,and Neuner [21],autobiographical memory can be described in terms of two types:1)cold memories,which comprise the knowledge about life events,and 2)hot memories,which comprise the emotional and sensory aspects of the experienced events.When the individual faces an extremely stressful or traumatic event,fight or flight responses are disabled,leaving the victim with only a startling freeze status.Further,the structures in the medial temporal lobe,which function as the portal for autobiographical memory,are believed to be altered such that hot and cold memories lose their interconnectivity.Elbert and colleagues [21] hypothesized that it is this disconnection between hot and cold memories that leads to individuals experiencing flashbacks entangled in fear and anxiety and makes the person unable to place these flashbacks in time and place.Restoring this connection can alleviate the horror of remembering the traumatic event,which is the essence of the NET work[21].
1.2.Context, objectives and hypotheses
The NET principles are consistent with the World Health Organization’s recommendations of a stepped care system to address mental health service gaps in developing countries [22].Specifically,the most effective,yet least resource-intensive treatment,is delivered first to strengthen the capacity of individuals,families,psychosocial service providers,and primary health care providers to address the basic mental health needs of the populace.Being a safe,feasible,and relatively short intervention [23],having the ability to address multiple traumas,considering the individual’s entire life journey in the therapy [24],and the need for less professional training [25] are some of the characteristics that make NET superior to other interventions for PTSD.Evidence on the effectiveness of NET is promising but not conclusive.A metaanalysis of randomized controlled trials that tested psychological interventions for PTSD and depression in refugees[26]showed that NET was effective for young refugees with positive outcomes that remained stable over a 12-month follow-up.However,a recent network meta-analysis failed to show a significant effect of NET for PTSD symptoms at post-intervention.Yet,NET appeared more effective than treatment as usual(defined as any intervention that reflects the usual care in a given treatment setting)in the subgroup of studies conducted in high-income countries[27].In low-income countries and post-conflict regions,few studies on the efficacy of NET have been conducted,and those were limited to populations from Iraq,Cario,and Saudi Arabia [28-30].There is a need to expand the current evidence base for NET in low-resource settings before drawing firm conclusions on its overall beneficial effects.
Jordan hosts an estimated 665,000 Syrian refugees,with 85%living below the poverty line on an income of approximately 96 USD per individual per month.The country faces challenges meeting their needs due to its small size,limited economic resources,burdened health infrastructure,and dwindling water supply [31,32].Researchers have examined several characteristics of Syrian refugees in Jordan,including psychosocial health,challenges,and the prevalence of PTSD and depression [33-35].However,no studies have examined how certain therapies work with PTSD among this population.In settings like Jordan,there is an overwhelming lack of access to trained professionals and resources,making NET a promising approach.Yet,the therapy needs to be adapted in terms of language and cultural appropriateness for the value of further research to be established.Therefore,the overarching purpose of this study was to evaluate the feasibility and preliminary efficacy of NET in reducing symptoms of trauma,depression,and anxiety among Syrian refugees residing in Jordan.We expect that participants assigned to receive NET will exhibit a positive response to the intervention protocol,perceive it as culturally appropriate,and actively participate in the majority of the therapy sessions.We also expect that,compared to those who were waitlisted,participants who received NET will show a greater reduction in PTSD symptoms as well as lower rates of co-occurring depression and anxiety.The findings from this study hold significant relevance in enhancing our understanding of evidence-based treatments for refugees in Jordan,and therefore,have the potential to inform the development of treatment programs in similar contexts.
2.Methods
2.1.Design
The research protocol received full review and approval from the institutional review board of the corresponding author’s institution,as well as the recruitment setting.Written informed consent was obtained from all participants.A two-arm randomized controlled trial (RCT) was implemented with 40 participants who were randomly assigned to the NET intervention (n=20) and a waitlisted control group (n=20).After the intervention,a purposive sample of six participants was selected for in-depth interviews aimed at capturing their perspectives and experiences regarding the intervention.
2.2.Participants
Participants in the study were required to meet specific criteria,including being at least 18 years old,having a diagnosis of PTSD from a psychiatrist using a structured diagnostic interview,and being willing to share personal feelings and experiences.Individuals who had a dual psychiatric diagnosis,except for anxiety and depression,had a cognitive disability,had speech or hearing problems,received the same intervention previously,or were undergoing another active psychotherapy at the time of the study were excluded.
The 10 NET sessions were conducted at the Jordanian Psychological Sciences Association (PSA) building in Amman,the capital.This NGO provides physical,psychological,and social services for Jordanians and refugees in Jordan.However,at the time of the current study,the activities and services of this NGO had been halted due to the COVID-19 pandemic,as the NGO relies on international funding,which was stopped amid the pandemic.A designated room was fully prepared to conduct the sessions.It had convenient access,simple decoration,was calm,and provided a private space to discuss sensitive issues.All sessions for all participants occurred in the same setting.A list of 65 de-identified potential participants,along with specific descriptors requested by the researchers to ensure eligibility,was provided by the NGO.Of them,15 were excluded[non-Syrian(n=7),have dual psychiatric diagnoses (n=5),previously received NET (n=2),on antidepressant medication (n=1)],leaving a total of 50 eligible participants.All 50 participants were contacted through the NGO and informed that there would be a random selection to participate in the study.Of them,40 participants agreed to participate and were randomly assigned to the trial arms.
2.3.Intervention
The hypothesis guiding NET is that those who frame their lives around the traumatic event often experience persistent trauma and distress,while those who frame the traumatic event within their lives can more easily recover [16].Thus,the goal of NET was to contextualize the sensory,affective,and cognitive memories of trauma within the client’s life course.The therapist and the client together created a timeline of the client’s life.A chronological elaboration for this timeline was then conducted over the subsequent sessions.Both important negative and positive life events were pinpointed and discussed [18].The client was assisted in reporting the traumatic event with extensive details and repeated exposures until it no longer induces anxiety.In addition,the therapist encouraged the client to express his/her emotions during each recall,aiming to habituate both emotions and physiological reactions during the sessions while also reconstructing cognitive defects from the traumatic event(s) [16].In the meantime,the therapist created written materials for the client’s autobiography,which helped the client to take control of their own life and political issues that have impacted them.The NET protocol of this study followed Schauer,Elbert,and Neuner guidelines[18].Weekly sessions were conducted for each participant,and each session lasted between 60 and 120 min.The number of conducted sessions was ten on average and these were arranged as follows.
Session I:During this critical session,the beginnings of a trusting relationship were established with the participant,a consent form was obtained,and participants filled in the demographic data sheet.Psychoeducation was also delivered on NET,including defining PTSD,types of traumas,factors that could exacerbate PTSD,and the fear cascade system.
Session II: Participants were asked to build a lifeline since childhood,identifying the major life events as they perceived them and using symbolic objects(stones or flowers)to attach to each life event (a flower for the positive/happy event and a stone for the negative/painful event).Detailed descriptions of any events were avoided,and the focus was solely on generalized titles of the events.Fig.1 is an example of a lifeline for one of the participants.
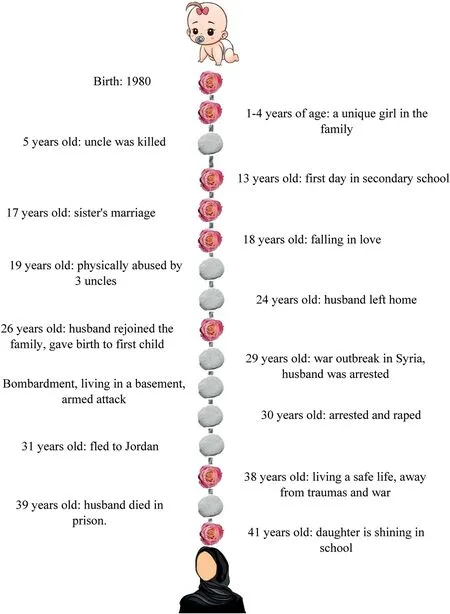
Fig.1.A lifeline example.
Session III to pre-final session: Over these sessions,participants described their memories in detail for all life events portrayed on the lifeline.In addition,at the beginning of each session,the therapist narrated what the participants reported in the previous sessions to gain validation and make any needed adjustments or corrections to the lifeline.The most important aspect of these sessions was to not end them before ascertaining that the participants were relieved of the symptoms associated with past traumatic event(s).According to the theory of Schauer,Elbert,and Neuner[18],clients who demonstrate improvements in emotional state and shift their attention toward the external environment are indicators for moving beyond exposure.The therapist carefully observed these states and shifts.In addition,participants were asked to express their emotions and report when they felt settled and ready to end the session.As recommended,no discussions around the traumatic events were initiated unless there was enough time to share all feelings surrounding [36].The major traumatic event,when present,was discussed during a dedicated individual session,with a strong emphasis on providing a comprehensive account of the event.
Final session: Upon near completion of NET,participants were asked to rebuild their lifeline and show how their perceptions regarding life events might have changed (i.e.,replacing some stones with flowers).In addition,they completed post-test questionnaires.Participants with no schooling received appropriate assistance from trained research personnel to ensure a fair and accurate completion of the questionnaires.Finally,the participant’s whole story was narrated,and they were given the chance to title their story.A hard copy of that story was given to each participant to strengthen and enrich their personal identity throughout their life journey.
The waitlist control group consisted of 20 participants who were given the opportunity to obtain the intervention after completion of the study.Some researchers recommend providing another intervention to the control group while they wait,so that they experience some benefit and/or to minimize the effect of no interaction with the control group.Thus,participants on the waitlist received an educational lecture about positive child-rearing practices.
2.4.Outcomes and measures
Being a feasibility study,retention rate,adherence to the study protocol,data completeness,cultural congruence,and participants satisfaction were considered primary outcome indicators.Additionally,we examined preliminary efficacy of NET on three psychological outcomes,including PTSD,depression,and anxiety symptoms,all of which were assessed at baseline and upon study completion.
PTSD symptoms were assessed using the Arabic version of the Harvard Trauma Questionnaire(HTQ-16)[37].The HTQ contains 16 items that measure PTSD symptoms,which are intrusion,avoidance,arousal,and hypervigilance.Responses range from 1 (never experienced during the past week) to 4 (extremely experienced during the past week)[38].The HTQ has been translated into many languages and showed satisfactory psychometric properties when examined for the Arabic,Farsi,Serbo-Croatian,Russian,and English versions.Internal consistencies for the Arabic version ranged from 0.74 to 0.89[37].The cut-off score for PTSD symptoms is 2 out of 4[38].The Cronbach’s α cooficient for the HTQ in this study was 0.77.
Depression and anxiety symptoms were collected using the Arabic version of Hopkins Symptoms Checklist-25 (HSCL-25) [39].The HSCL-25 contains 25 items that measure symptoms of anxiety and depression.The first 10 items assess the level of anxiety and the remaining 15 items assess the level of depression.Individual responses range from 1(never experienced during the past week)to 4 (extremely experienced during the past week) [40].The cut-off scores are 2.1 and 2.0 out of 4 for depression and anxiety symptoms,respectively [40].The Arabic version of HSCL-25 was validated among 214 Lebanese participants with an internal consistency of 0.73[39].Cronbach’s α cooficient for the HSCL-25 in this study was 0.70 and 0.88 for anxiety and depression subscales,respectively.
2.5.Sample size
The required sample size for this pilot study was calculated based on a statistical test of difference between two independent means (groups).The effect size was estimated based on prior published pilot studies on NET among refugees.The reported effect sizes for NET seemed to be high for PTSD as well as depression and anxiety symptoms.A study by Zang and colleagues[41]reported an effect size of 0.8 and 0.9 for pre-and post-PTSD and depressive symptoms effects,respectively.However,another study [42] reported that the size of the treatment effect on post-traumatic symptoms at post-test was large (1.09-1.35).We followed the recommendation of Wilker and colleagues [17] to base the effect size calculation on a conservative estimate of 0.8.For this study to test the hypothesis that those who received NET will show a significant reduction in PTSD,anxiety,and depression symptoms compared to those who were waitlisted,a one-sided α level was set at 0.05,with a power level of 0.8,and an effect size of 0.8.Accordingly,we needed to enroll 42 subjects(n=21 per group)in the present study.
2.6.Randomization
Following the CONSORT statement,participants in this study were randomly allocated to the two arms of the trial using a computer-generated allocation list with 1∶1 allocation to either the NET intervention group or the waitlist control group.The randomization was applied by a research assistant who was blind to the allocation process using sequentially numbered,opaque,and sealed envelopes.The envelopes remained sealed to ensure concealment of the sequence of treatment allocations from the research team.Upon participant assignment to the trial,the respective envelope was unsealed,revealing the assigned allocation.Due to the nature of the intervention,neither participants nor the therapist could be blinded.However,participants were instructed not to reveal any information related to the group that they had been assigned to or regarding the therapeutic process.All sessions were organized and applied by the first author(NS),who is certified in NET and has extensive training in its use among refugees.A certified NET trainer also supervised the sessions’ delivery to ensure treatment fidelity.Measures were also taken to avoid attrition and drop-out from the study.Participants received compensation for the transportation cost.Having the therapy conducted by a therapist of similar national origin to the participants increased the cultural acceptance of the intervention and the likelihood that the participant would show up for the sessions.
2.7.Data collection and analysis
The data for this study was collected by a research assistant who was blind to the RCT arms,and the entire process took place at the same center where the intervention was conducted.This data collection occurred on a one-to-one basis,with each participant being assigned a specific time to attend and complete the study questionnaire in a designated room within the same center.This approach was adopted to ensure a controlled and consistent environment for all participants.The collected data underwent a rigorous analysis using IBM’s Statistical Package for Social Sciences(SPSS 21) to ensure validity and reliability.Initially,a comprehensive univariate analysis was performed,scrutinizing each variable independently to assess data quality.Potential missing data was addressed,and a multivariate diagnostic test(Little,1988)was used to evaluate the randomness of these omissions.The analysis revealed that the missing data followed a pattern completely at random (P>0.05).The average percentage of missing ranged between 1%and 5%across all the items of the study measures.Given the data’s missing completely random nature,missing scores were imputed using the median of the non-missing items.Analyses were conducted both with the unimputed and imputed datasets,revealing no significant differences (allP>0.05).Lastly,nondirectional statistical tests were performed with a significance level set at 0.05 for each test.Descriptive statistics were employed to characterize the sample and survey data.Independentt-tests were conducted to assess mean score differences in PTSD,anxiety,and depression between the intervention and control groups.In light of the exploratory nature of the study,no adjustment for multiple tests was made regarding the level of significance.
3.Results
3.1.Participants’ characteristics
All participants (n=40) were Syrian refugees diagnosed with PTSD,with a mean age of 37.5 years (range 18-64;SD=12).The majority(n=30)were female and married(n=24).Approximately half of the participants (n=18) had an elementary level of education,and 36 were unemployed.Table 1 details the participants’characteristics.There were no significant statistical differences between the intervention and control groups regarding age,gender,marital status,employment,or educational level.Nearly half of the participants (n=17) had a medical diagnosis,including hypertension (n=7) and diabetes (n=6).Of those with a medical diagnosis,13 were diagnosed while residing in Jordan.All participants were exposed to multiple traumas,including witnessing or experiencing a family member being brutally arrested (n=29),witnessing or experiencing a bombardment (n=25),seeing the deformed body of a relative (n=16),and witnessing or experiencing torture (n=13).
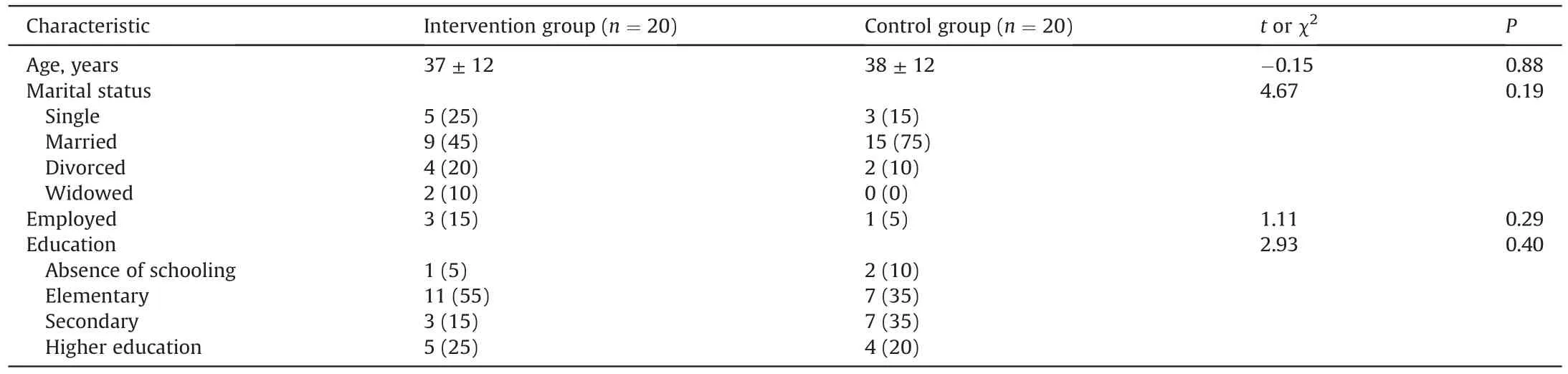
Table 1 Participants characteristics.
3.2.Feasibility results
Multiple indicators were collectively assessed to determine the feasibility of the intervention.The results pertaining to retention rate,adherence to the study protocol,data completeness,cultural congruence,and participants’satisfaction provided strong support for the future implementation of the full-scale RCT.Having the intervention delivered by members of the same religious and ethnic community with shared language and culture has aided NET’s acceptability among participants,especially as many of them were victims of those perceived as authority figures.In this respect,it is worth noting that all participants committed to all NET sessions with no dropouts,which is unusual with refugee samples given their unstable circumstances.This feasibility study considered issues that often prevent attendance,including travel costs,breach of registration status confidentiality,inconsideration of culturalnorms,and fear of consequences of not participating [43,44].The study also yielded a high level of data completeness with minimal data missing,contributing to the robustness of the study’s feasibility findings.Feedback from participants indicated a high level of satisfaction with their involvement in the NET.Participants reported feeling valued,respected,and well-supported throughout the trial.Participants also recommended applying NET with other refugees,and many asserted that NET would be even more helpful if it was applied to them shortly after they reached Jordan in order to help them vent their feelings and move forward instead of having their lives fixated around the trauma.This positive feedback suggests that the trial procedures and interventions were wellreceived,further supporting the feasibility of conducting the NET.Further in-depth descriptions of participants’ experience and satisfaction with the intervention,as reported during the follow-up interviews,were reported elsewhere[45].
3.3.Baseline and post-intervention analyses: differences and effect sizes
We initially conducted independentt-tests to compare baseline mean scores of PTSD,anxiety,and depression between the intervention and control groups (Table 2).The results revealed no statistically significant differences in PTSD and anxiety scores,implying comparable baseline conditions.However,a significant difference emerged in depression scores (t=2.65,P<0.05),with the intervention group scoring higher.

Table 2 PTSD,anxiety,and depression symptoms at baseline and comparison between the two groups.
Subsequently,we performed independent t-tests to assess mean differences in PTSD,anxiety,and depression scores between the intervention and control groups following NET.The analysis disclosed significant differences,with the intervention group displaying significantly lower mean scores in PTSD symptoms,anxiety,and depression compared to the control group(Table 3).Effect sizes ranged from medium to large,signifying the practical significance of these findings.

Table 3 Post-intervention differences in PTSD,anxiety,and depression symptoms between the intervention and control group.
4.Discussion
The overarching purpose of this study was to evaluate the feasibility and preliminary efficacy of NET in reducing symptoms of trauma,depression,and anxiety among Syrian refugees residing in Jordan.To investigate this aim,an RCT was utilized,and 40 Syrian refugees were randomly assigned to either a group receiving the NET,or a waitlist control group.This study found that NET was feasible and acceptable.Further,for all three efficacy outcomes -symptoms of PTSD,depression,and anxiety -there was a statistically and clinically significant reduction in symptoms after NET compared to a waitlist control.
These findings are consistent with previous studies supporting the effectiveness of NET in reducing PTSD symptom severity with various study populations and trauma types [46-48].In a metaanalysis of seven trials [49],the average effect size was medium(0.63) for all studies,and 0.53 for studies in which interventions were delivered by trained graduate students.Likewise,these findings underscore previous studies that have demonstrated NET is effective in managing symptoms of anxiety and depression[15,50,51],including studies that have documented clinical significance of NET [50].
The fact that this study supported the effectiveness of NET in reducing symptoms of depression and anxiety is particularly important for health care providers because these symptoms cooccur in most patients diagnosed with PTSD.The participants in our study were no different.While it is difficult to accurately delineate the temporality of the relationships among the three symptoms,given the lack of any longitudinal data on the participants,findings from previous studies show that it is often PTSD that provokes symptoms of anxiety and depression [52,53].Therefore,using therapies like NET is promising as it handles traumatic events as well as the associated depressive and anxiety symptoms.
4.1.Where to go from here?
Given the large numbers of refugees worldwide,topics related to refugees’ mental health should be included in higher education curricula,particularly in programs that teach public health,mental health,and nursing.Training and equipping mental health professionals with the knowledge and skills needed to administer quality NET sessions and manage referrals is recommended.Data show that all levels of mental health providers can successfully provide NET,and this approach should be considered in all settings that engage individuals with trauma histories,given that there remains a dearth of mental health services compared to the need.We believe that psychiatric nurses are best suited to be trained on NET.Psychiatric nurses are often the frontline for mental healthcrises,and they frequently have intensive contact with patients.This contact enables psychiatric nurses to be the first to observe changes during NET that allows them to respond accordingly to restore,maintain,and/or promote their patients’mental health and well-being.Improving access to NET through psychiatric nurses may have a promising role in bridging the mental health services gap in low-resource settings.
The COVID-19 pandemic highlighted the important role of online psychological support and tele-mental health services to address gaps in care.Online treatments can overcome the challenges often experienced in face-to-face treatments,such as the stigma associated with attending a mental health care facility,poor access to treatment in rural/remote areas,travel expenses,and confidentiality/privacy issues.Kaltenbach and colleagues provided practical guidelines for online NET application for PTSD,with the goal of empowering therapists working with trauma patients to conduct e-NET confidently and safely[54].More work needs to be done to establish e-NET as a viable option for treating PTSD and associated mood disorders.This includes conducting trials to compare outcomes of e-NET with in-person NET among refugees and other survivors of trauma.
4.2.Limitations
Findings from this study must be considered within the context of its limitations.First,depression scores for participants in the intervention group were already significantly higher at baseline than their controls.Baseline differences may potentially indicate that the randomization process was not successful in creating comparable groups.This may compromise the ability to attribute the observed effects solely to the treatment under investigation.Second,the study utilized a pre-posttest design,hindering the evaluation of how long the benefits lasted and whether symptoms returned.Third,the data collection occurred in the middle of the COVID-19 pandemic,which might have affected the psychological state of the involved participants.Other limitations include the sample being relatively small,its preponderance of females,and the majority being unemployed,possibly related to the outcomes found.
5.Conclusions
While this study has several methodological limitations prohibiting solid conclusions from being drawn,considering the findings together with available evidence from existing relevant RCTs suggest that offering NET for Syrian refugees in Jordan is likely to be affordable and sustainable.Findings also provide promising evidence that,relative to no treatment,NET can be promising in reducing symptoms of PTSD,depression,and anxiety among refugees.It is worth mentioning that in this study,symptoms of PTSD,depression,and anxiety were all reduced immediately post NET,though more often reduction is observed within a frame of three months after the treatment.A longitudinal investigation with several follow up assessment points post-treatment would boost the validity of the findings,including whether NET is useful for long-term improvements in mental health among Syrian refugees in Jordan and other similar contexts.Given the scarcity of mental health resources respective to need in Jordan,our findings suggest that NET could be included in the mental health services provided for refugees and patients with PTSD in clinics,hospitals,and other NGOs as part of ongoing quality improvement.Meantime,future research should directly compare NET with established traumafocused therapies to clarify whether NET is uniquely beneficial for refugees and trauma survivors.Closer research on whether different trauma types need different interventions is also warranted.
Funding
This study was funded by the University of Jordan Deanship of Scientific Research.
CRediT authorship contribution statement
Nadeen Smaik:Conceptualization,Methodology,Investigation,Writing -reviewing and editing.Leigh Ann Simmons:Conceptualization,Methodology,Writing-reviewing and editing.Bayan Abdulhaq:Conceptualization,Methodology,Writing -reviewing and editing.Latefa Ali Dardass:Conceptualization,Methodology,Supervision,Writing -reviewing and editing.
Declaration of competing interest
All authors have seen and approved the final version of the manuscript being submitted,and we have no conflicts of interest to report.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2023.09.007.
 International Journal of Nursing Sciences2023年4期
International Journal of Nursing Sciences2023年4期
- International Journal of Nursing Sciences的其它文章
- The associations among nurse work engagement,job satisfaction,quality of care,and intent to leave: A national survey in the United States
- 《國際護理科學(英文)》2024年征稿
- Meaning of community activity participation for older adults in couple households
- The implementation and impacts of national standards forcomprehensive care in acute care hospitals: An integrative review
- Nurse-coordinated home-based cardiac rehabilitation for patients with heart failure: A scoping review
- Effectiveness of a family-based program for post-stroke patients and families: A cluster randomized controlled trial