
Comparison of different preoperative objective nutritional indices for evaluating 30-d mortality and complications after liver transplantation
2024-03-07 03:09ChuanLiHongXiaChenYanHuaLai
Chuan Li,Hong-Xia Chen,Yan-Hua Lai
Abstract BACKGROUND The nutritional status is closely related to the prognosis of liver transplant recipients,but few studies have reported the role of preoperative objective nutritional indices in predicting liver transplant outcomes.AIM To compare the predictive value of various preoperative objective nutritional indicators for determining 30-d mortality and complications following liver transplantation (LT).METHODS A retrospective analysis was conducted on 162 recipients who underwent LT at our institution from December 2019 to June 2022.RESULTS This study identified several independent risk factors associated with 30-d mortality,including blood loss,the prognostic nutritional index (PNI),the nutritional risk index (NRI),and the control nutritional status.The 30-d mortality rate was 8.6%.Blood loss,the NRI,and the PNI were found to be independent risk factors for the occurrence of severe postoperative complications.The NRI achieved the highest prediction values for 30-d mortality [area under the curve (AUC)=0.861,P < 0.001] and severe complications (AUC=0.643,P=0.011).Compared to those in the high NRI group,the low patients in the NRI group had lower preoperative body mass index and prealbumin and albumin levels,as well as higher alanine aminotransferase and total bilirubin levels,Model for End-stage Liver Disease scores and prothrombin time (P < 0.05).Furthermore,the group with a low NRI exhibited significantly greater incidences of intraabdominal bleeding,primary graft nonfunction,and mortality.CONCLUSION The NRI has good predictive value for 30-d mortality and severe complications following LT.The NRI could be an effective tool for transplant surgeons to evaluate perioperative nutritional risk and develop relevant nutritional therapy.
Key Words: Liver transplantation;Nutritional indicator;Complications;Prognosis;Nutrition assessment
lNTRODUCTlON
Liver transplantation (LT) is considered to be the most effective and definitive treatment option for patients suffering from end-stage liver disease.These conditions provide these patients with the opportunity not only to survive but also to extend their lifespan significantly.However,the occurrence of posttransplant complications remains prevalent and can greatly influence postoperative prognosis.This can largely be attributed to the compromised preoperative state of liver transplant recipients and the intricate nature of the surgical procedure.Recently,there has been increasing recognition of the critical roles played by preoperative nutrition and immune status in modulating surgical outcomes.
The serum prealbumin concentration,which can objectively reflect nutritional status and is almost unaffected by external supplementation,is an accurate biomarker for assessing the severity of liver disease.It can also be used for preoperative nutritional assessment and risk stratification[1-4].The controlling nutritional status (CONUT),prognostic nutritional status index (PNI),and nutritional risk index (NRI) are widely used objective indicators for evaluating nutritional status.These indicators are associated not only with cancer-related complications but also with the long-term prognosis of cancer patients[5-10].However,few studies have investigated the role of these nutritional indices in predicting liver transplant outcomes.Therefore,this study delves into this matter.
MATERlALS AND METHODS
Patient characteristics
This study was approved by the Ethics Committee of the People's Hospital of Guangxi Zhuang Autonomous Region.The inclusion criteria were as follows: (1) First-time liver transplant recipients aged 18-65 years;(2) Organ donation from deceased citizens;and (3) Complete clinical data.The exclusion criteria were: (1) Multiple organ transplants;(2) Severe pneumonia or severe cardiovascular and cerebrovascular diseases before surgery;(3) Receiving marginal livers[11];or (4) Incomplete follow-up data.This study was approved by the ethics committee of the People's Hospital of Guangxi Zhuang Autonomous Region (KY-ZC-2023-056).All patients provided written informed consent for data analysis before transplantation.
Study design
Before performing a LT,patient demographic information,which include age,sex,body mass index (BMI),and relevant medical history,such as hypertension,diabetes,and hepatitis B,were collected.Additionally,donor age,graft weight,and various laboratory values,such as prealbumin,albumin (ALB),lymphocyte count,alanine aminotransferase (ALT),aspartate aminotransferase,total bilirubin,and creatinine,were collected.The Model for End-Stage Liver Disease (MELD) score,total cholesterol level,type of donor liver,prothrombin time (PT),and platelet count are also important factors to consider.During LT,data such as operating time,anhepatic phase time,total ischemic time,intraoperative blood loss,and intraoperative urine output were collected.After LT,the incidences of pneumonia,abdominal infection,abdominal bleeding,graft rejection,primary graft nonfunction,early graft dysfunction,severe complications (Clavien-Dindo grade ≥ 3),bile leakage,biliary stricture and mortality within 30 d were recorded.
Complications above Grade III include various conditions such as portal vein stenosis,portal vein thrombosis,hepatic artery stenosis,hepatic artery thrombosis,bile leakage,bile duct stenosis,retransplantation,pleural effusion requiring thoracentesis,peritoneal effusion requiring peritoneal puncture,intra-abdominal hemorrhage,respiratory failure necessitating extracorporeal membrane oxygenation support,liver insufficiency requiring artificial external liver support,renal failure requiring hemodialysis treatment,intracranial hemorrhage,and mortality.
The CONUT score consists of three components: The serum ALB concentration,total cholesterol concentration,and lymphocyte count[12].The PNI can be calculated using the formula: ALB (g/L)+5 × lymphocyte count (× 109/mL).The following equation was used to determine the NRI: (1.519 × ALB,g/L)+(41.7 × actual body weight/ideal body weight)[13].The ideal weight for males and females can be calculated as follows: For males,2.3 kg per foot is added to a base weight of 50 kg (if height > 5 feet,with 1 foot equal to 30.48 cm);for females,1.65 kg per foot is added to a base weight of 48.67 kg (if height > 5 feet,with 1 foot equal to 30.48 cm)[14].If the actual weight exceeds the ideal weight,set the ratio to one[15].
This study aimed to analyze the risk factors associated with severe postoperative complications (Clavien-Dindo grade ≥ 3) and 30-d mortality following LT.Moreover,the researchers compared the effectiveness of the CONUT score,NRI,PNI,and prealbumin concentration as predictors of postoperative complications and mortality after LT using receiver operating characteristic (ROC) curves.Based on the area under the curve (AUC),the most accurate predictive index was identified and utilized to stratify patients into low-risk and high-risk groups using an appropriate cutoff value.Furthermore,the study compared the differences in baseline characteristics and postoperative complications between the two groups.
Postoperative assessment
After transplantation surgery and before discharge,the functionality of the transplant was assessed through routine laboratory tests.Surgical complications are typically diagnosed by evaluating clinical symptoms and conducting diagnostic examinations.These postoperative complications were documented in the patients' medical records.The Clavien-Dindo classification system was employed to assess and classify these complications.In this study,complications classified as Clavien-Dindo III or higher were considered severe.We recorded all adverse reactions,including pneumonia,abdominal infection,abdominal bleeding,graft rejection,primary graft nonfunction,early graft dysfunction,death,biliary leakage,and biliary stricture,in patients after surgery.
Statistical analysis
The statistical analysis was performed using SPSS 23.0 software.Continuous variables are represented using the median,25thpercentile,and 75thpercentile,while categorical variables are represented using the frequency.A binary logistic regression model was used for both univariate and multivariate analyses of the entire sample.In the univariate analysis,indicators with a significance level ofP< 0.05 were included in the multivariate analysis.However,given the existence of multicollinearity between the serum ALB concentration and the NRI,PNI,and CONUT score,the total serum ALB concentration was not incorporated into the multivariate analysis.The diagnostic results of multicollinearity,following the exclusion of ALB,indicated that the values for the variance inflation factor were less than 5.Consequently,no collinearity issues were observed within the model.The predictive values,optimal thresholds,sensitivities,and specificities for complications and mortality were calculated using ROC curves and AUC.MedCalc 10.2 software was used for the Z test,and the Delong test was used to compare the AUC of the different scoring systems.APvalue of less than 0.05 was considered to indicate statistical significance.
RESULTS
Patient characteristics
A total of 162 patients were included in the study,including 133 males and 29 females.Fourteen patients (8.6%) died within a 30-d period following LT.The median age of the patients was 53.0 (45.0-57.0) years.The preoperative BMI was recorded as 23.0 (21.1-25.1).Preoperative hypertension was observed in 18 patients,diabetes was present in 22 patients,and 118 patients tested positive for hepatitis B surface antigen (Table 1).

Table 1 Patient characteristics
Univariate and multivariate analyses of severe complications and mortality
The factors correlated with the 30-d mortality rate are outlined in Table 2.Univariate analysis revealed that the following factors were significantly correlated with 30-d mortality: BMI,operation time,blood loss,intraoperative urine volume,prealbumin concentration,NRI,CONUT,PNI,ALT,total bilirubin,preoperative MELD score,and PT.The multivariate analysis confirmed that blood loss [odds ratio (OR)=1.001,95%CI: 1.000-1.002,P=0.034],the NRI (OR=0.665,95%CI: 0.446-0.991,P=0.045),the CONUT (OR=2.088,95%CI: 1.016-4.291,P=0.045),and the PNI (OR=0.920,95%CI: 0.848-0.997,P=0.042) were risk factors for the 30-d mortality rate (Table 2).

Table 2 Univariate and multivariate analyses of predictors of 30-d mortality
Factors associated with severe complications (Clavien-Dindo grade ≥ 3) included operation time,blood loss,intraoperative urine volume,NRI,PNI,ALB,total bilirubin,preoperative MELD score,and PT.However,the results of the multivariate analysis showed that blood loss (OR=1.003,95%CI: 1.001-1.005,P=0.004),the NRI (OR=0.942,95%CI: 0.901-0.986,P=0.011),and the PNI (OR=0.994,95%CI: 0.989-0.999,P=0.013) were risk factors associated with severe complications (Clavien-Dindo grade ≥ 3;Table 3).

Table 3 Factors that predict a Clavien-Dindo grade ≥ 3

Table 4 Values of different preoperative objective nutritional indicators for predicting 30-d mortality

Table 5 Comparisons of the area under the curve of various nutritional indicators for predicting severe complications and 30-d mortality

Table 6 Values of different preoperative objective nutritional indicators for predicting severe complications

Table 7 Comparation of the clinical characteristics among different nutritional risk index groups

Table 8 Comparison of postoperative complications between the low nutritional risk index group and the high nutritional risk index group,n (%)
The value of different preoperative objective nutritional indicators for predicting severe complications and mortality
ROC curve analysis revealed that the NRI,CONUT score,PNI,and prealbumin concentration were significantly associated with 30-d mortality (P< 0.05).Among these,the NRI had the highest AUC value (0.861) for prediction (Tables 4 and 5,Figure 1).When the predictive ability of various indicators for severe complications was compared,the NRI,PNI,and prealbumin concentration all showed good predictive value for severe complications (P< 0.05).Among them,the NRI exhibited the highest predictive ability (AUC=0.643;Tables 5 and 6,Figure 2).

Figure 1 Receiver operating characteristic curve for the cutoff values of multiple preoperative objective nutritional indicators for predicting postoperative death. CONUT: Control nutritional status;PNI: Prognostic nutritional index;NRI: Nutritional risk index;AUC: Area under the curve.
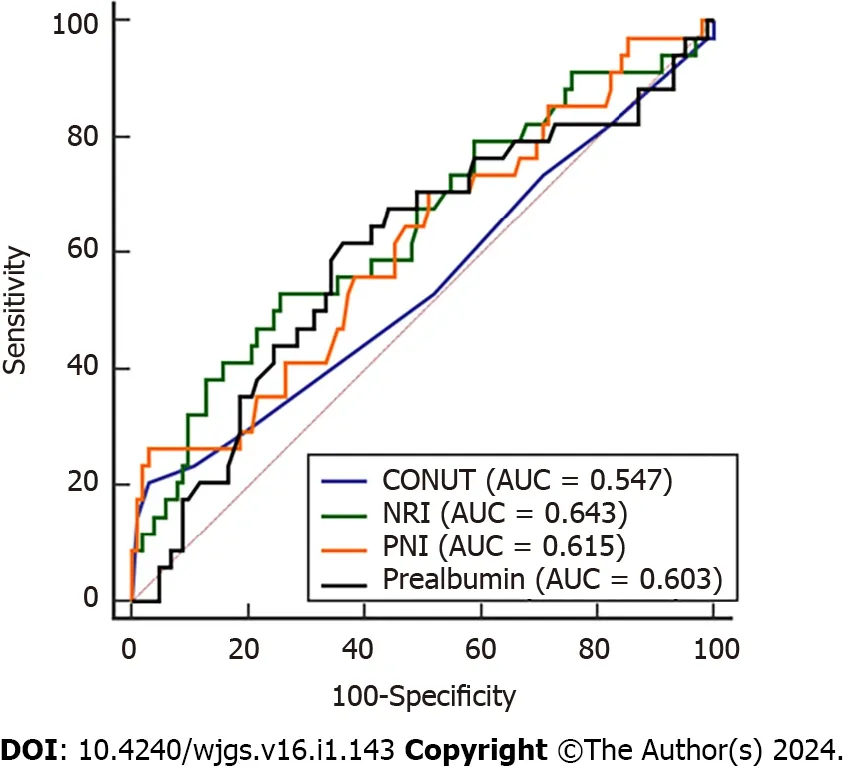
Figure 2 Receiver operating characteristic curve for the cutoff values of multiple preoperative objective nutritional indicators for predicting severe complications. CONUT: Control nutritional status;PNI: Prognostic nutritional index;NRI: Nutritional risk index;AUC: Area under the curve.
Comparison of clinical characteristics and postoperative complications between the high NRI group and low NRI group patients
In terms of clinical characteristics,the high NRI group exhibited a greater BMI,improved liver function,and a lower preoperative MELD score than did the low NRI group.In terms of prognosis,the high NRI group had a significantly lower incidence of postoperative intra-abdominal bleeding,primary graft dysfunction,and 30-d mortality than did the low NRI group (P< 0.05).These findings are summarized in Tables 7 and 8.
DlSCUSSlON
Early posttransplant mortality is the main factor affecting the overall effectiveness of LT,with most recipients dying within 1 mo after LT.In the current situation of severe shortage of donor livers and an increasing number of patients awaiting for LT,there is an urgent need for ideal risk prediction models to evaluate posttransplantation effectiveness and further determine the patients who are most likely to benefit from LT.
The MELD score is extensively applied in clinical practice and successfully predicts the likelihood of mortality in patients awaiting LT,as well as the risk of mortality after the transplant procedure[16,17].However,the MELD score itself has limitations,as research has shown that it does not predict perioperative outcomes well in liver cancer patients without cirrhosis[18,19].In recent years,scholars have shown greater interest in the relationship between nutritional status and post-LT complications.The serum prealbumin concentration serves as a reliable marker of liver synthesis capacity and nutritional status,making it a useful tool for predicting long-term survival in liver cancer patients undergoing liver resection[20].Recent research has shown that prealbumin also demonstrates significant superiority in predicting complications after LT (AUC=0.754)[1].The COUNT score,PNI,and NRI are commonly used inflammatory nutritional indices in clinical practice.The CONUT score is a measure of the immune-nutritional status of patients and has beenreported to independently predict the prognosis of various malignant tumors[21].Among liver transplant patients,those with intermediate to high CONUT scores have a higher incidence of postoperative Clavien-Dindo grade III/IV complications and infections than do those with high CONUT scores[22].The PNI has a certain role in predicting post-LT renal injury and postliver cancer recurrence[23,24].The NRI was first introduced in 2005 as an objective nutritional assessment tool that accurately predicts the mortality rate of elderly patients in internal medicine[25].Subsequent multicenter studies have demonstrated that patients with an NRI of 98 or lower have a 1.5-fold greater risk of postoperative complications following abdominal surgery than patients with an NRI above 98.However,to date,the relationship between the NRI and post-LT complications has not been thoroughly elucidated[26].Therefore,we further investigated the relationship between nutritional indices and the prognosis of LT patients.
This retrospective analysis revealed that the NRI,PNI,and prealbumin have certain value for predicting 30-d mortality and severe complications in liver transplant recipients,with the NRI having the highest AUC value.The CONUT score can predict 30-d mortality in liver transplant recipients but cannot predict severe postoperative complications.In the multifactorial logistic regression analysis,blood loss,NRI,PNI,and CONUT were independent predictors of 30-d mortality,while blood loss,NRI,and PNI were independent predictors of severe postoperative complications.Based on the optimal cutoff value of the NRI,patients with an NRI > 88 had better preoperative liver function;lower rates of intraabdominal bleeding (6.1%vs20.0%,P=0.025) and primary graft nonfunction (1.5%vs10.0%,P=0.044);and lower mortality rates (6.1%vs20.0%,P=0.025) than patients with an NRI < 88.
The serum prealbumin concentration has good predictive ability for 30-d mortality and severe complications after LT,consistent with previous findings[1].The variation in AUC values may be attributed to varying definitions of severe complications.Serum prealbumin is a carrier protein entirely produced by liver cells,and its main physiological function is to transport thyroid hormones and vitamin A,enhancing the body's immune function by promoting lymphocyte maturation[27].Moreover,due to its short half-life and small amount of interference factors,prealbumin can sensitively reflect liver synthesis function and has high sensitivity and specificity for detecting hepatocyte damage[28,29].Therefore,the serum prealbumin concentration can be a potential indicator for predicting poor early outcomes after LT.
We found that the AUC for predicting 30-d mortality was the highest for the NRI,followed by the PNI,CONUT,and prealbumin concentration.Similarly,the AUC for predicting severe complications was the highest for the NRI,followed by the PNI and prealbumin concentration.Although both the NRI and the PNI incorporate the measurement of ALB,the NRI also reflects the degree of weight loss in patients.Malnutrition is prevalent among patients with end-stage liver disease,and the incidence of malnutrition in individuals with decompensated cirrhosis and liver failure ranges from 50% to 90%[30].Surgical intervention exacerbates liver injury,reduces ALB synthesis,impairs immune function and body repair capacity,increases the likelihood of postoperative complications,and adversely affects survival prognosis in malnourished patients.Recent studies have elucidated the association between sarcopenia and the prognosis of liver transplant recipients[22,31].These findings indicate that diminished muscle mass is linked to unfavorable outcomes following LT and is a predictive factor for short-term survival.Furthermore,low muscle mass has an equally significant impact on the prognosis of patients with malignancies.In patients with nonmetastatic breast cancer,the overall mortality rate is significantly greater in individuals with sarcopenia (hazard ratio,1.41;95%CI,1.18-1.69)[32].Similarly,among patients diagnosed with colorectal cancer,those exhibiting sarcopenia have a notably elevated overall mortality rate (hazard ratio,1.27;95%CI,1.09-1.48) compared to that of their counterparts without sarcopenia[33].This finding suggested a strong association between wasting and unfavorable prognosis.However,the existing evidence is insufficient to establish a definitive link between lymphocyte count and nutritional status.Consequently,the predictive efficacy of the NRI surpasses that of the PNI,highlighting its potential in clinical prognostication.The CONUT score incorporates cholesterol as an indicator.Cholesterol is primarily synthesized in the liver,and its levels indirectly reflect liver synthetic function.Changes in liver function due to cellular damage can lead to alterations in cholesterol levels.Although a smallscale study suggested an association between low cholesterol levels and unsuccessful liver transplant,there is currently insufficient evidence to support the role of cholesterol in the prognosis following LT[34].Therefore,these findings may explain why the predictive efficacy of the CONUT score is lower than that of the NRI and PNI.
This study aimed to compare the role of multiple objective nutritional indicators in predicting the prognosis of LT patients,thereby facilitating a comprehensive preoperative nutritional assessment,early identification of malnutrition,timely and appropriate nutritional support for enhancing surgical safety,and reducing the incidence of postoperative complications.This study has several limitations,including the following: (1) The sample size was not large enough;(2) This was a retrospective analysis,and further prospective analysis is needed to clarify the predictive value of different scoring systems for post-LT outcomes;and (3) We analyzed only a portion of the nutritional indicators and did not include all nutritional indicators in our analysis.Despite these limitations,our results still demonstrate the superiority of the NRI as a nutritional indicator for predicting post-LT 30-d mortality and severe complications.
CONCLUSlON
This study identified several independent risk factors associated with 30-d mortality,including blood loss,the PNI,the NRI,and the CONUT.The 30-d mortality rate was 8.6%.Blood loss,the NRI,and the PNI were found to be independent risk factors for the occurrence of severe postoperative complications.The NRI achieved the highest predictive values for 30-d mortality (AUC=0.861,P< 0.001) and severe complications (AUC=0.643,P=0.011).Compared to those in the high NRI group,the patients in the low NRI group had lower preoperative BMIs;prealbumin,and ALT levels;and higher ALT,total bilirubin,MELD score,and PT (P< 0.05).Furthermore,the low NRI group exhibited significantly greater incidences of intraabdominal bleeding,primary graft nonfunction,and mortality.In conclusion,the NRI can serve as an effective tool for transplant surgeons to assess perioperative nutritional risk in patients and formulate relevant nutritional interventions.
ARTlCLE HlGHLlGHTS
Research background
Nutritional status is closely associated with the prognosis of liver transplantation (LT) patients.
Research motivation
However,few studies have thoroughly investigated the relationship between the preoperative nutritional status of liver transplant recipients and postoperative prognosis.In clinical practice,there is a lack of a simple and effective tool for assessing the nutritional risk of patients during the perioperative period and for predicting the outcomes of LT.
Research objectives
The objective of this study was to compare the value of different preoperative objective nutritional indicators for predicting the 30-d mortality and the incidence of complications following LT.
Research methods
This study conducted a retrospective analysis of clinical data from 162 patients who underwent LT.The present study compared the ability of the serum prealbumin concentration,the controlling nutritional status (CONUT) score,the prognostic nutritional index (PNI),and the nutritional risk index (NRI) to predict the 30-d mortality rate and the incidence of severe complications after LT.This study also aimed to analyze the risk factors associated with the 30-d mortality rate and incidence of severe complications after LT.The area under the receiver operating characteristic curve was used to select the index with the best predictive ability.Patients were then divided into low-risk and high-risk groups based on the optimal cutoff value,and the differences in postoperative complications and mortality rates between the two groups were compared.
Research results
This study identified several independent risk factors associated with 30-d mortality,including blood loss,the PNI,the NRI,and the CONUT.The 30-d mortality rate was 8.6%.Blood loss,the NRI,and the PNI were found to be independent risk factors for the occurrence of severe postoperative complications.The NRI achieved the highest prediction values for 30-d mortality [area under the curve (AUC)=0.861,P< 0.001] and severe complications (AUC=0.643,P=0.011).Compared to those in the high NRI group,the patients in the low NRI group had lower preoperative body mass index and prealbumin and albumin levels,as well as higher alanine aminotransferase and total bilirubin levels,Model for Endstage Liver Disease scores and prothrombin time (P< 0.05).Furthermore,the group with a low NRI exhibited significantly greater incidences of intraabdominal bleeding,primary graft nonfunction,and mortality.
Research conclusions
The NRI has good predictive value for 30-d mortality and severe complications following LT.The NRI could be an effective tool for transplant surgeons to evaluate the perioperative nutritional risk and provide relevant nutritional therapy.
Research perspectives
The purpose of this study was to investigate the predictive value of different objective nutritional indicators before surgery for the outcome of LT.
FOOTNOTES
Author contributions:Li C conceived the study,collected and analyzed the data and drafted the manuscript;Chen HC assisted with the data collection;Lai YH revised the manuscript;and all the authors read and approved the final version to be published.
Supported byThe Self-Funded Research Project of the Health Commission of Guangxi Zhuang Autonomous Region,No.Z-A20230045.
lnstitutional review board statement:The study was reviewed and approved by the Ethics Committee of Guangxi Zhuang Autonomous Region People's Hospital,No.KY-ZC-2023-056.
lnformed consent statement:All patients provided written informed consent for data analysis before transplantation.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Chuan Li 0000-0002-8193-4352;Yan-Hua Lai 0000-0002-9474-6350.
S-Editor:Li L
L-Editor:A
P-Editor:Li L
 World Journal of Gastrointestinal Surgery2024年1期
World Journal of Gastrointestinal Surgery2024年1期
- World Journal of Gastrointestinal Surgery的其它文章
- Prospects in the application of ultrasensitive chromosomal aneuploidy detection in precancerous lesions of gastric cancer
- Prognostic value of ultrasound in early arterial complications post liver transplant
- Added value of ratio of cross diameters of the appendix in ultrasound diagnosis of acute appendicitis
- Single-incision laparoscopic transabdominal preperitoneal repair in the treatment of adult female patients with inguinal hernia
- Predictive value of machine learning models for lymph node metastasis in gastric cancer: A two-center study
- Micro-power negative pressure wound technique reduces risk of incision infection following loop ileostomy closure