
Micro-power negative pressure wound technique reduces risk of incision infection following loop ileostomy closure
2024-03-07 02:28DengYongXuBingJunBaiLinaShanHuiYanWeiDengFengLinYaWangDaWang
Deng-Yong Xu,Bing-Jun Bai,Lina Shan,Hui-Yan Wei,Deng-Feng Lin,Ya Wang,Da Wang
Abstract BACKGROUND Prophylactic loop ileostomy is an effective way to reduce the clinical severity of anastomotic leakage following radical resection of rectal cancer.Incisional surgical site infection (SSI) is a common complication after ileostomy closure.AIM To evaluate the efficacy and safety of the micro-power negative pressure wound technique (MPNPWT) in preventing incisional SSI.METHODS This was a prospective,randomized controlled clinical trial conducted at a single center.A total of 101 consecutive patients who underwent ileostomy closure after rectal cancer surgery with a prophylactic ileostomy were enrolled from January 2019 to December 2021.Patients were randomly allocated into an MPNPWT group and a control group.The MPNPWT group underwent intermittent suturing of the surgical incision with 2-0 Prolene and was covered with a micro-power negative pressure dressing.The surgical outcomes were compared between the MPNPWT (n=50) and control (n=51) groups.Risk factors for incisional SSI were identified using logistic regression.RESULTS There were no differences in baseline characteristics between the MPNPWT (n=50) and control groups (n=51).The incisional SSI rate was significantly higher in the control group than in the MPNPWT group (15.7% vs 2.0%,P=0.031).However,MPNPWT did not affect other surgical outcomes,including intra-abdominal complications,operative time,and blood loss.Postoperative hospital stay length and hospitalization costs did not differ significantly between the two groups (P=0.069 and 0.843,respectively).None of the patients experienced adverse effects of MPNPWT,including skin allergy,dermatitis,and pain.MPNPWT also helped heal the infected incision.Our study indicated that MPNPWT was an independent protective factor [odds ratio (OR)=0.005,P=0.025)] and diabetes was a risk factor (OR=26.575,P=0.029) for incisional SSI.CONCLUSION MPNPWT is an effective and safe way to prevent incisional SSI after loop ileostomy closure.
Key Words: Micro-power negative pressure technique;Ileostomy closure;Incisional surgical site infection;Infection prevention;Postoperative incision
lNTRODUCTlON
Prophylactic loop ileostomy is an effective way to reduce the clinical severity of anastomotic leakage following radical resection for rectal cancer[1].Afterward,the digestive tract can be reconstructed through ileostomy closure.Although ileostomy closure is technically easy,it is associated with a non-negligible overall morbidity rate (11%-37%),with incisional surgical site infection (SSI) being the most common[2].Incisional SSI is responsible for increased pain,longer hospital stays,and higher treatment costs.Surgeons have attempted to implement effective techniques to prevent incisional SSI.For example,purse-string skin closure is used as a substitute for conventional linear skin closure[3],and subcutaneous closedsuction drainage or negative-pressure technology (NPT) has been introduced to achieve adequate drainage[4].These are valid techniques but have some limitations.Purse-string skin closure results in a circular open incision that requires frequent dressing changes.Applying a subcutaneous suction drain or a negative-pressure system has an adverse effect on patient mobility.
The micro-power negative pressure wound technique (MPNPWT) is a new approach to wound treatment in China[5].This technique is based on a wound dressing that is made of a special polyvinyl alcohol foam material.When covering the wound,the material is completely sealed with a medical transparent film.Thus,a closed environment is formed at the local wound.Then,this kind of medical,biological material can produce the "siphonic effect" and "pumping effect" through compression,thus generating micro-power negative pressure that can quickly absorb exudates from the wound surface and achieve wound drainage (Figure 1).The micro-power negative pressure dressing can spare frequent dressing changes or an external device.This technique has been successfully applied in wound healing[6-8].It reduces wound edema and stimulates epithelial cell proliferation and granulation tissue growth,thus shortening wound healing time.However,it is seldom used in the postoperative incisions to prevent incisional SSI.According to our previous experience with MPNPWT in patients with loop ileostomy closure,the postoperative incision could heal satisfactorily.

Figure 1 Composition and working principle of micro-power negative pressure wound technique.A: The wound dressing is made of a special polyvinyl alcohol foam material.The material covers the wound and is sealed by a medical transparent film.In this way,it becomes a three-layer dressing containing a medical film layer,liquid locking layer,and micro-power vacuum and pumping effect layer;B: When exudates are absorbed into the liquid locking layer,the dressing expands,and the medical film layer is elevated.Then the closed space becomes larger and forms a local micro-power vacuum,which exerts negative pressure attraction on the wound and its deep soft tissue.
The primary objective of this prospective,randomized controlled trial (RCT) was to evaluate the efficacy and safety of MPNPWT in preventing incisional SSI after loop ileostomy closure.
MATERlALS AND METHODS
Study design
This was a single-center prospective,RCT conducted at Sir Run Run Shaw Hospital,Hang Zhou,China,between January 2019 and December 2021.The trial was registered at Chinese Clinical Trial Registry (registration number: ChiCTR-2200064827) after approval by the Ethics Committee of Sir Run Run Shaw Hospital,School of Medicine,Zhejiang University (No.20191217-9).Each participant provided written informed consent prior to study enrollment.This work is reported in line with the CONSORT guidelines.
Patients
Patients were enrolled according to the following inclusion criteria: (1) Age over 18 years;(2) history of radical resection of a rectal tumor with protective loop ileostomy;(3) scheduled to undergo an elective procedure of ileostomy closure;and (4) provision of signed informed consent.The exclusion criteria were as follows: (1) Age < 18 years;(2) loop ileostomy due to other surgeries;(3) end ileostomy;(4) emergency surgery;(5) other surgical procedures performed during the ileostomy period;and (6) no provision of informed consent.Patients can withdraw from the study without any reason or condition.The enrolled patients were randomly assigned to either an MPNPWT or a control group using sealed envelopes.
Sample size
The sample size calculation was based on an unpublished prospective observational study conducted at our center,in which 38 patients were evaluated for incision SSI after ileostomy.The overall incidence of incisional SSI was 10.5%.Incisional SSI occurred in four of the 25 patients (16%) in the control group,while no incisional SSI was observed in 13 patients using MPNPWT (incisional SSI incidence was 0).A total of 44 patients were required in each group to achieve a type I error of 0.05 with a power of 0.8.Assuming a 10% dropout rate,the expected 50 patients were recruited in each arm,with a sample size of 100 patients.
Randomization and blinding
An independent statistician randomly assigned eligible patients in a 1:1 ratio using sequentially sealed envelopes to the control or MPNPWT groups without stratification.Randomization was done after admission to the hospital and before ileostomy closure.The sealed envelopes contained allocations from a computer-generated table of random numbers and were opened before surgery.This study did not permit the use of blinding methods because the application of the MPNPWT could not be concealed.However,the analysis was done by a blinded statistician.
Surgical procedures
Each patient underwent the same procedure of ileostomy closure at the Department of Colorectal Surgery,Sir Run Run Shaw Hospital.During the operation,the ileum was reconstructed with mechanical side-to-side anastomosis using an easyEndoTMendoscopic linear cutter stapler (60 mm length,blue cartridge).Hand-sewn end-to-end anastomosis can also be chosen.All patients received reinforcement sutures for anastomotic stoma.The fascia of the rectus abdominis muscle was closed using continuous suturing.The subcutaneous tissues were not sutured.The skin was intermittently sutured with 2–0 Prolene in both groups.Needle spacing was 6–8 mm in the control group and 10–12 mm in the MPNPWT group.A micro-power negative pressure dressing (MJ-01B3,Guangdong Meiji Biotechnology Co.Ltd.) was filled on the skin surface of the patients in the MPNPWT group by nurses from the wound care clinic.As displayed in Figure 2,the incision was covered with two pieces of polyvinyl alcohol foam material and then sealed and fixed with a transparent film.The material expanded as it absorbed exudates.The dressing was removed after 72 h.If excessive exudates caused negative pressure failure,the dressing was removed earlier and changed to a new one.

Figure 2 lncision equipped with micro-power negative pressure wound dressing. A: During the surgery,the incision was intermittently sutured with 2-0 Prolene with a 10-12 mm needle spacing in the micro-power negative pressure wound technique group;B: Then the micro-power negative pressure wound dressing was equipped immediately;C: When exudates were absorbed,they appeared on the the material’s surface,and the dressing expanded;D: A clean and dry incision was obtained after removing the material in 72 h.
Perioperative and postoperative care
Cefmetazole was administered intravenously as a preoperative prophylactic antibiotic.Etimicin sulfate was injected in patients allergic to penicillin or cephalosporin.Typically,the same antibiotics were used postoperatively until the Creactive protein dropped below 50 mg/L (usually three continuous days).If there was other evidence of infection,the type and duration of antibiotics were adjusted according to clinical experience.In the experimental group,the micropower negative-pressure dressing was maintained for 72 h and then changed to a traditional dressing material.The negative pressure dressing should be replaced if there was excessive leakage or if the negative pressure failed within 72 h.In the control group,the traditional dressing material was routinely changed in 72 h.In addition,the dressing was changed whenever it became wet.The stitches were removed 2 wk after surgery in both groups.The patients were followed for 30 d postoperatively.The surgical wounds were routinely monitored by the surgical team for 30 d.
Identification of incisional SSI
The primary outcome of this study was incisional SSI.The infection occurred within 30 d after the operation and involved only the skin or subcutaneous tissue of the incision.It was defined according to the standard of the Center for Disease Control and Prevention (1999)[9],following at least one of the criteria: Purulent drainage,with or without positive culture;laboratory confirmation of the incision exudate;or any one of the following signs or symptoms of infection: Pain or tenderness,localized swelling,and redness or heat.
Statistical analysis
Continuous variables with a normal or non-normal distribution are presented as the mean ± SD or median and 25th–75thpercentiles,respectively.Continuous variables were compared using Student'st-test or Mann–WhitneyUtest.Categorical variables were compared using Pearson's chi-squared test or Fisher's exact test.Logistic regression was used to detect risk factors for incisional SSI.Statistical significance was set atP< 0.05.The data were statistically analyzed using SPSS software (version 25.0.0.2;SPSS Inc.,Chicago,IL,United States).
RESULTS
Characteristics of patients
This study enrolled 101 consecutive patients: 51 in the control group and 50 in the MPNPWT group (Figure 3).Table 1 displays no significant differences in the demographic and clinical features of the patients between the two groups.Most enrolled patients were male (65.3%).Most patients were in good health,with an average body mass index within the normal range for Chinese people (18.5–24).The majority had an American Society of Anaesthesiology (ASA) score of 1-2 (96.0%),with normal values of preoperative albumin and hemoglobin.There were no significant differences in the medical history,including hypertension and diabetes,between the two groups.Since a considerable proportion of patients received perioperative chemoradiotherapy,the waiting time until ileostomy closure was almost 6 mo.
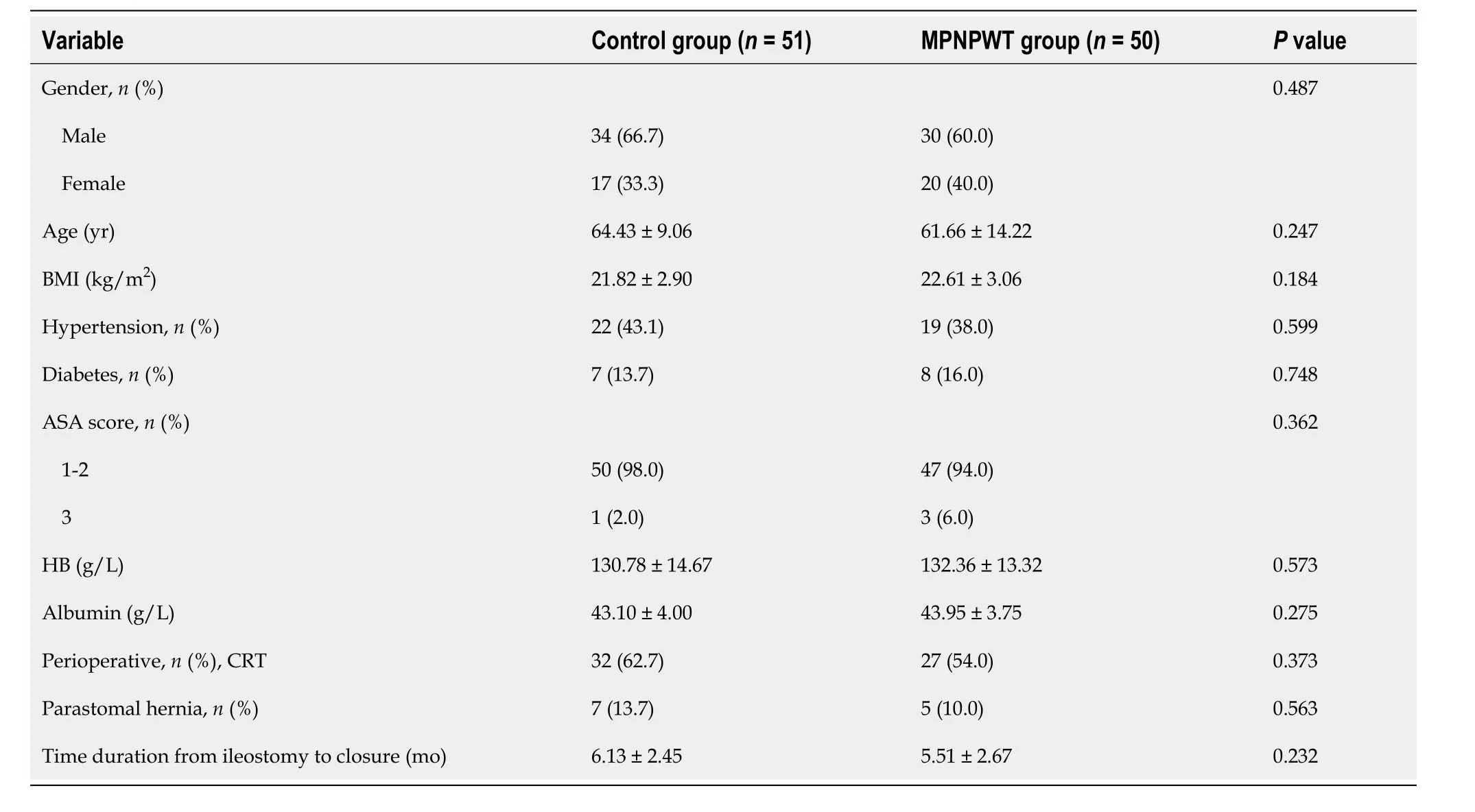
Table 1 Demographic and clinical features of included patients
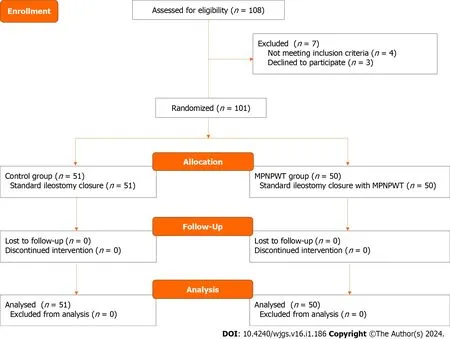
Figure 3 Consort diagram.
Surgical outcomes
We compared the surgical outcomes between the two groups to evaluate the efficacy and safety of MPNPWT.The surgical outcomes did not differ significantly between them (Table 2).These two different surgical procedures shared similar operative time (78.14 ± 20.02vs81.36 ± 17.64,P=0.393) and blood loss (17.35 ± 4.40vs19.70 ± 7.45,P=0.056) in the control and MPNPWT groups.Moreover,postoperative intra-abdominal complications,including anastomotic inflammation and bowel obstruction,did not differ significantly between the two groups.No anastomotic leakage or bleeding was observed in either group.The patients complained of no pain or discomfort with a micro-power negative pressure dressing.In addition,in the MPNPWT group,no patients had skin allergy or dermatitis potentially caused by the micro-power negative pressure dressing.The above evidence indicates that MPNPWT is a safe procedure without side effects on ileostomy closure.
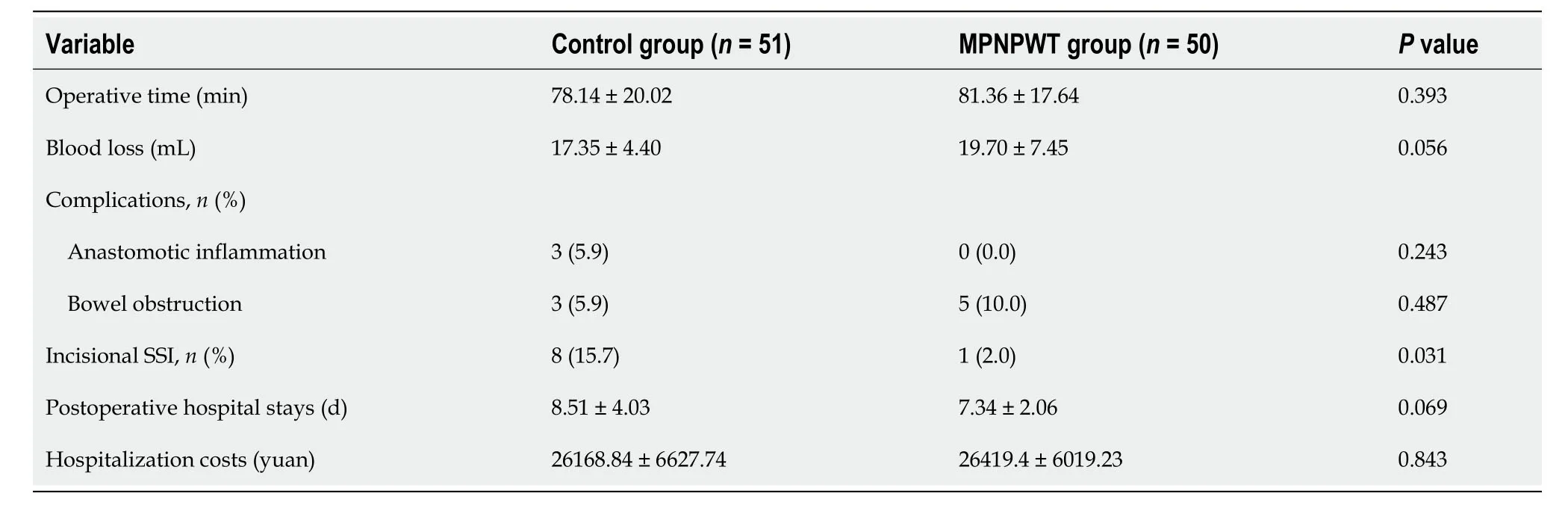
Table 2 Surgical outcomes of included patients
Importantly,the incisional SSI rate was significantly lower in the MPNPWT group than in the control group (2.0%vs15.7%,P=0.031).In the MPNPWT group,only one patient developed SSI on postoperative day 5.However,eightpatients in the control group experienced incisional SSI within 9 d after surgery.Three patients underwent MPNPWT after opening the infected incision.The incisions were then cleaned and subsequently closed.In addition,there were 15 patients with a medical history of diabetes.The incisional SSI rate among diabetic patients was lower in the MPNPWT group (1/8) than in the control group (3/7),but the difference was not statistically significant (12.5%vs42.9%,P=0.282).Postoperative hospital stay length and hospitalization cost did not differ significantly between the two groups (P=0.069 and 0.843,respectively).
Risk factors for incisional SSI
Logistic regression was performed to identify the risk factors associated with incisional SSI.Table 3 shows that those patients who underwent ileostomy closure with MPNPWT had a significantly lower incisional SSI rate than those who underwent traditional procedures [odds ratio (OR)=0.110,P=0.041)].Moreover,patients with diabetes were more likely to suffer incisional SSI (OR=5.891,P=0.017).Multivariate analysis further confirmed that MPNPWT was an independent protective factor (OR=0.005,P=0.025) and diabetes was a risk factor (OR=26.575,P=0.029) for incisional SSI.
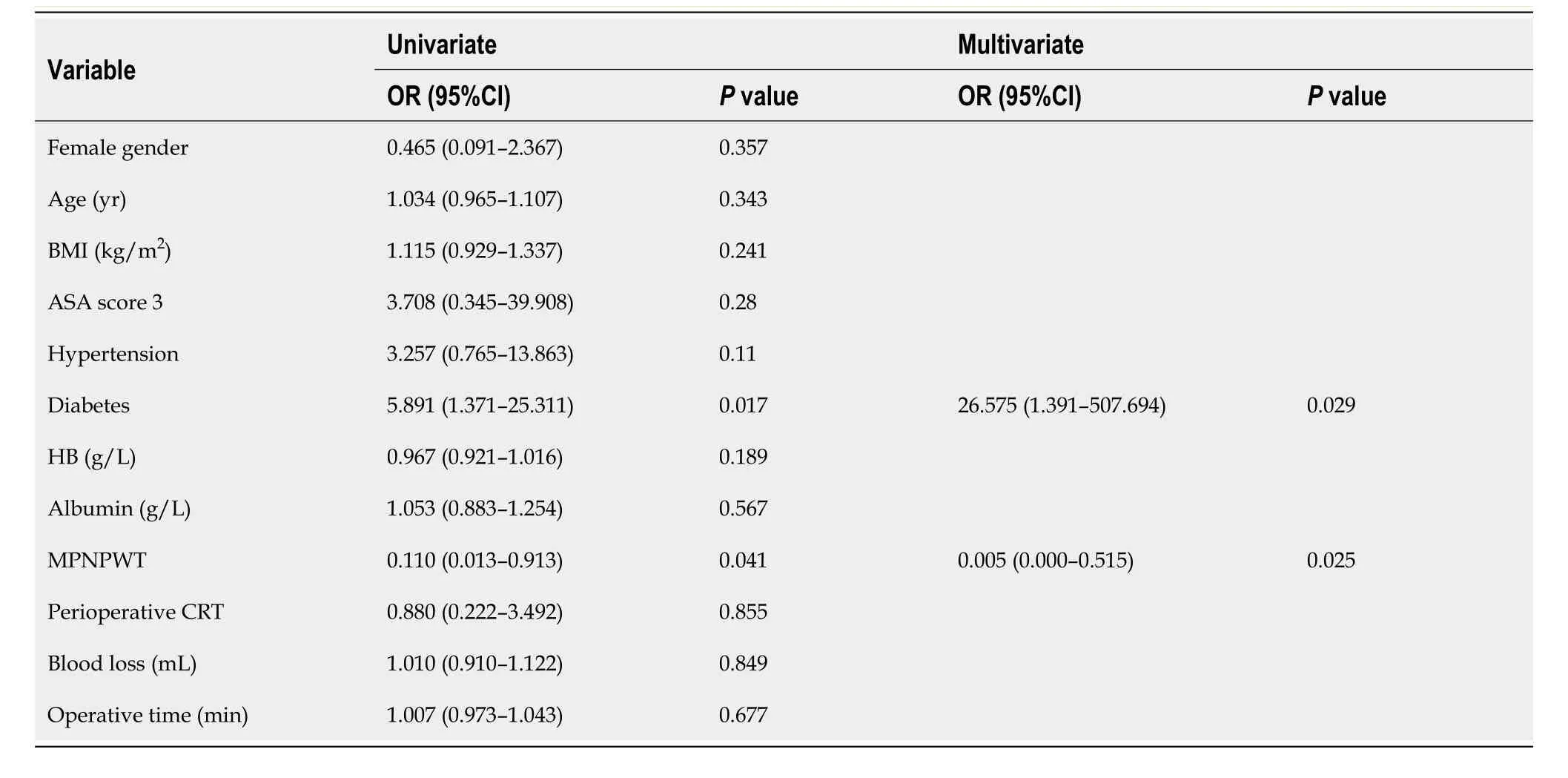
Table 3 Logistic analysis of risk factors for surgical site infection
DlSCUSSlON
Incisional SSI is the main complication of loop ileostomy closure.In the present study,we introduced a new technique,MPNPWT,to prevent postoperative incision infection after loop ileostomy closure.This technique significantly reduced the incisional SSI rate to a low level (2.0%).
Surgical incisions are classified into four classes.Class I or class II wounds are clean or relatively clean,with an infection risk of < 2% or < 10%,respectively[10].Although the surgical incision for ileostomy closure is a class II wound,the incisional SSI rate is much higher than those of other intestinal surgeries,ranging from 2% to 40%[11-13].In this study,the incisional SSI rate in the control group was also higher than 10%.Adequate drainage is the most effective way to deal with an infected or potentially infected incision and can greatly reduce the incisional SSI rate[14].Current methods for incisional SSI prevention involve increasing drainage,including subcutaneous suction drainage,negativepressure system,and purse-string skin closure.However,each of these technologies has its limitations.
MPNPWT is a new technique that has been improved by the NPT.It does not require the configuration of external negative pressure equipment,whether connected to the wall or portable.The suction efficiency of traditional NPT depends on pressure regulation.If the negative pressure is too low,it may be unable to absorb the effusion effectively,yet if it is too high,it may cause tissue damage.Moreover,high pressure may induce the exfoliation of regenerative cells in the wound[15].However,MPNPWT uses a special material that produces micro-negative pressure by absorbing exudates rather than a suction device.The material expands when the exudates are absorbed.Then,the medical film is gradually elevated,leading to a larger closed space and local vacuum,resulting in a negative pressure suction effect.The suction mechanism is different from the capillary action caused by the adhesive and cohesive forces interacting between the liquid and the surface.Due to the unique design of the material,the more exudates it absorbs,the more powerful the micro-negative pressure.Obviously,excess exudates can invalidate the negative pressure.Meanwhile,it only maintains a relatively low pressure (–0.1 to–0.3 kPa) that may not cause tissue damage.Consequently,MPNPWT can be used to prevent incisional infection because it works on incisions with exudates.The liquid-locking layer of the material has a high liquid absorption efficiency.According to the test,a material with 7.0 cm × 10 cm × 0.1 cm dimension can absorb and preserve up to 70 mL of liquid[6].After applying MPNPWT to the incision,the exudate may be quickly absorbed by the liquid-locking layer,thereby keeping the incision clean.In the MPNPWT group,we used 2–0 Prolene to close the incision with a wide needle distance so that the micro-negative pressure could effectively absorb the effusion and create a favorable condition for incision healing.
In this study,the MPNPWT group had a 2.0% incisional SSI rate,which was significantly lower than that of the control group.Moreover,MPNPWT may be superior to other techniques in preventing incision infection[3,13,16-18].Serracantet al[13] inserted contralateral drainage into the subcutaneous space to reduce the incisional SSI rate after loop ileostomy closure,achieving an 8.6% rate in 35 patients.Wierdaket al[18] designed a RCT to assess the role of prophylactic negative-pressure wound therapy in preventing wound healing complications.In that study,negativepressure wound therapy reduced the incidence of SSI to 5.71%.Another study by Leeet al[3] introduced a purse-string skin closure in which a circular suture was performed on the dermal layer with absorbable sutures.Purse-string skin closure contributed to a significantly lower wound infection rate (5.6%) than conventional linear skin closure.Although the incisional SSI rate may vary among studies,it is presumed that MPNPWT is a more efficient and convenient technique.A recent RCT study recruited patients undergoing reoperative open colorectal resections to investigate the effect of NPT on SSIs[19].The results indicated that the 30-d SSI rate did not differ significantly between the NPT group and control groups (9.4%vs14.1%,P=0.28).Therefore,that study concluded that NPT was unrelated to a significant reduction in SSI.There were several reasons for this contradictory conclusion.First,the high SSI rate in the NPT group could be explained by the selection criteria that included high-risk factors for SSI.Second,we have noticed that the incision was closed with skin staples in that study.Generally,the needle spacing of skin staples was narrower than that of Prolene,which might lead to poor drainage.Moreover,the narrow needle spacing would cause the epidermis to heal earlier than the subcutaneous tissue,which might prevent NPT from absorbing exudates.Therefore,our MPNPWT accompanied with wider needle spacing would be more effective for incisional SSI.
Several factors are associated with incisional SSI,such as ASA score and operative time[9].Diabetes is likely to induce poor wound healing.Our results demonstrated that diabetes was an independent risk factor for incisional SSI.Moreover,MPNPWT could decrease the incisional SSI rate in diabetic patients.Additionally,MPNPWT was appropriate for infected incisions.Patients with MPNPWT spared the trouble of dressing change and suffered less pain than patients with open incisions.Previous studies have confirmed the efficacy of MPNPWT in open wounds such as diabetic foot,open fracture,and burn wounds[6,8].Notably,MPNPWT is not recommended for wounds with excessive exudates because of the special mechanism of this material.
In our center,we do not choose subcutaneous suction drainage or purse-string skin closure to prevent incisional SSI.We believe that these techniques are cumbersome and increase patient suffering.In contrast,MPNPWT is simple and convenient.It can be performed in a post-anesthesia care unit by a wound care clinic at our center or performed by trained surgeons during the surgery.Furthermore,we confirmed that MPNPWT is safe.Specifically,patients in the MPNPWT group did not suffer from skin allergy,dermatitis,or any pain.In addition,MPNPWT did not affect hospitalization costs (P=0.843).Moreover,MPNPWT shortened the length of hospital stays to a certain extent,though not significantly.Surgical outcomes such as operative time,hospitalization cost,and length of hospital stay are important factors associated with patient recovery and feelings.Previous studies have often lacked investigations into these aspects.Leeet al[3] reported that the median hospitalization period in the purse-string skin closure group was 7 d,which was significantly shorter than that in the linear skin closure group.However,according to our center's experience,it takes longer than 7 d to heal the incision with purse-string skin closure,implying that patients still need dressing changes even after hospital discharge.
The main limitation of this study was that it was a single-center clinical trial with a relatively small sample size.In addition,needle spacing was different between the two groups,which may be a bias when analyzing the effectiveness of MPNPWT.Finally,some other less significant confounders that were not recorded in our study may have introduced bias.A larger multicenter clinical study with a better design should be conducted in the future.
CONCLUSlON
As a prospective RCT,our study introduced a novel technique,MPNPWT,to prevent incisional SSI after loop ileostomy closure.MPNPWT reduces the incidence of incisional SSI and helps patients recover during hospitalization.
ARTlCLE HlGHLlGHTS
Research background
Although ileostomy closure is technically easy,it is associated with a non-negligible overall morbidity rate (11%-37%),with incisional surgical site infection (SSI) being the most common.
Research motivation
The incisional SSI rate after ileostomy closure is much higher than those of other intestinal surgeries,ranging from 2% to 40%.Incisional SSI is responsible for increased pain,longer hospital stays,and higher treatment costs.Current methods for incisional SSI prevention have limitations.Finding a new approach to prevent incisional SSI is urgent for patients receiving ileostomy closure.
Research objectives
Micro-power negative pressure wound technique (MPNPWT) contains a special material that produces micro-negative pressure by absorbing exudates rather than suction device.It reduces wound edema and stimulates epithelial cell proliferation and granulation tissue growth,thus shortening wound healing time.This study aimed to evaluate the efficacy and safety of MPNPWT in preventing incisional SSI.The results of our study will provide foundation for future application of MPNPWT.
Research methods
This was a single-center,prospective,randomized controlled trial (RCT).An independent statistician randomly assigned eligible patients in a 1:1 ratio using sequentially sealed envelopes to a control group or an MPNPWT group without stratification.Micro-power negative pressure dressing was filled on the skin surface of patients in the MPNPWT group by nurses from wound care clinic.
Research results
MPNPWT significantly reduced incisional SSI rate (2.0%).MPNPWT is a safe technique without any side effect.MPNPWT could also help heal the infected incision.
Research conclusions
Our study introduces a novel technique,MPNPWT,to prevent incisional SSI after loop ileostomy closure.MPNPWT reduces the incidence of incisional SSI after loop ileostomy closure.
Research perspectives
A larger RCT with a larger sample is the direction of the future research.
FOOTNOTES
Author contributions:Xu DY and Bai BJ were responsible for the study conception and design;Shan LN and Wei HY analyzed the data and wrote the manuscript;Lin DF,Wang Y,and Wang D critically revised the article for important intellectual content;all the authors reviewed and approved the final version to be published.
Supported bythe Zhejiang Provincial Natural Science Foundation of China,No.LQ20H260002.
lnstitutional review board statement:The study was reviewed and approval by the Ethics Committee of Sir Run Run Shaw Hospital,School of Medicine,Zhejiang University (No.20191217-9).
Clinical trial registration statement:The trial was registered at Chinese Clinical Trial Registry at https://www.chictr.org.cn (registration number: ChiCTR2200064827).
lnformed consent statement:All study participants,or their legal guardian,provided informed written consent prior to study enrollment.
Conflict-of-interest statement:All authors declare no potential conflicting interests related to this paper.
Data sharing statement:No additional data are available.
CONSORT 2010 statement:The authors have read the CONSORT 2010 Statement,and the manuscript was prepared and revised according to the CONSORT 2010 Statement.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Deng-Yong Xu 0009-0004-3016-7829;Bing-Jun Bai 0000-0002-4545-0633;Lina Shan 0000-0001-9799-4352;Hui-Yan Wei 0000-0002-9128-1148;Da Wang 0000-0003-4955-8999.
S-Editor:Lin C
L-Editor:Wang TQ
P-Editor:Zhao S
 World Journal of Gastrointestinal Surgery2024年1期
World Journal of Gastrointestinal Surgery2024年1期
- World Journal of Gastrointestinal Surgery的其它文章
- Prospects in the application of ultrasensitive chromosomal aneuploidy detection in precancerous lesions of gastric cancer
- Prognostic value of ultrasound in early arterial complications post liver transplant
- Added value of ratio of cross diameters of the appendix in ultrasound diagnosis of acute appendicitis
- Single-incision laparoscopic transabdominal preperitoneal repair in the treatment of adult female patients with inguinal hernia
- Predictive value of machine learning models for lymph node metastasis in gastric cancer: A two-center study
- Unraveling the efficacy network: A network meta-analysis of adjuvant external beam radiation therapy methods after hepatectomy