
TCERG1L hypermethylation is a risk factor of diabetic retinopathy in Chinese children with type 1 diabetes
2024-03-20 06:33YuQianYingXiaoQiuRongLinZhaoYuXiangLiPuCuiJiaQiSunSiCongLiXinRanQinHaiDongZouChenHaoYangPeiYaoJin
Yu Qian, Ying Xiao, Qiu-Rong Lin, Zhao-Yu Xiang, Li-Pu Cui, Jia-Qi Sun, Si-Cong Li,Xin-Ran Qin, Hai-Dong Zou, Chen-Hao Yang, Pei-Yao Jin
1Department of Ophthalmology, Shanghai General Hospital,Shanghai Jiao Tong University School of Medicine, Shanghai First People’s Hospital, Shanghai 200080, China
2Shanghai Eye Diseases Prevention & Treatment Center,Shanghai Eye Hospital, Shanghai 200040, China
3National Clinical Research Center for Eye Diseases, Shanghai Clinical Research Center for Eye Diseases, Shanghai Key Clinical Specialty, Shanghai Key Laboratory of Ocular Fundus Diseases, Shanghai Engineering Center for Visual Science and Photomedicine, Shanghai Engineering Center for Precise Diagnosis and Treatment of Eye Diseases, Shanghai 200080,China
4Department of Ophthalmology, Children’s Hospital of Fudan University, Shanghai 201102, China
Abstract
● KEYWORDS: DNA methylation; 850K array; pyrosequencing;diabetic retinopathy; type 1 diabetes; children
INTRODUCTION
Type 1 diabetes mellitus (T1DM) is a complex disease resulting from the interplay of genetic, epigenetic, and environmental factors[1-2].Diabetic retinopathy (DR) is the most common and severe ocular complication of diabetes,and its pathogenesis has been studied extensively[3-4].DNA methylation, along with histone acetylation and micro ribonucleic acid dysregulation, is an important epigenetic phenomena that results in altered gene expression[5].Former researches indicated that DR is related with the DNA methylation changes of several genes[6-11].However, most of these former researches focused on type 2 diabetes patients,only two studies have reported a connection between DR and DNA methylation changes in T1DM adults[7-8].So far, no such study has been published in T1DM children.The prevalence of DR in T1DM children is relatively lower than that in adults,which may result from a shorter disease duration.However,studying DR related DNA methylation in T1DM children is essential, because it may provide reference for preventing DR development in an early stage, even before its onset.
Several former studies indicated that T1DM children without DR have a significantly thinner macular retinal thickness compared with their healthy contemporaries[12-15], which is consistent with our previous findings in our study population.Moreover, we also found that the macular retinal thickness of T1DM children without DR decreased during a one-year follow-up (data not published yet).Retina thinning before the occurrence of microvascular changes might be resulted from diabetic retinal neurodegeneration[16].Based on these evidences, we hypothesized that macular retina thinning could be used as a biomarker for early retinal damage related with T1DM before the onset of DR.Thus, in the present study,we first used the 850K BeadChip array to analyze the DNA methylation status of 40 T1DM children without DR, and screened for differential methylation sites (DMS) in the lowest 25% children with the thinnest macular retinal thickness comparing with the others.Four DMS with a potential role in diabetes were identified by the 850K BeadChip.Afterwards,we used the pyrosequencing assay to further investigate that four DMS in another study population of 27 T1DM children,including four with DR as case group, and the rest 23 without DR as controls.Thus, the DMS and their according genes related to the development of DR in T1DM children were obtained.
The aim of the present study was to identify the DMS and their according genes associated with DR development in T1DM children.This study may help to reveal novel DNA methylation markers, and to improve the current understanding, prevention and treatment of DR in T1DM patients.
SUBJECTS AND METHODS
Ethical ApprovalThis study was a part of the Shanghai Children and Adolescent DM Eye study (clinical trial registration number: NCT 03587948)[17], and it included two hospital-based surveys (conducted in 2019 and in 2021 separately).This study was conducted in accordance with the tenets of the Declaration of Helsinki, and was approved by the ethics committees of the Shanghai General Hospital affiliated to Shanghai Jiao Tong University School of Medicine and Children’s Hospital of Fudan University in Shanghai (approval number: 2016KY005 and LS No.01-2018, respectively).All of the participants and their guardians were fully informed about the procedures, and their informed consents were collected.
Setting and ParticipantsThe inclusion criteria were 1)age between 5y and 18y; 2) diagnosed with T1DM based on the World Health Organization diagnostic criteria[18]; 3) best corrected visual acuity no worse than 0.1 (logMAR visual acuity); 4) no previous eye surgery.Children with systemic diseases other than T1DM, and with severe eye diseases other than DR were excluded.Our research team consisted of three ophthalmologist, three optometrists, and 15 auxiliary staff.
Systemic and Ophthalmologic ExamsDetailed examination procedures were described previously[17].Briefly, participants’age, gender, diabetes duration, medication history, family history of diabetes, weight and height were collected though questionnaire.Body mass index (BMI) was calculated as weight/height2(kg/m2).Blood pressure was measured at the site.Routine blood tests results of the participants within 6mo at the hospital were collected.Total cholesterol and triglycerides were measured using an enzymatic assay.Hemoglobin A1C (HbA1c) was measured by ion exchange chromatography.
Comprehensive eye examinations were conducted in each of the participant in the ophthalmology clinic at Children’s Hospital of Fudan University.Patients’ eyelid, conjunctiva, cornea, iris,and lens were examined with a slit-lamp microscope (SL130;Zeiss, Germany), and the vitreous and fundus were examined with 90 D noncontact lens (90 D, Ocular, Bellevue, WA, USA)after cycloplegia.DR was diagnosed if microaneurysms,intraretinal hemorrhages, definite venous beading or prominent intraretinal microvascular abnormalities were observed[19].Visual acuity was measured using the international standard logMAR visual acuity chart.The intraocular pressure was measured by a non-contact tonometer (model NT-530P,Nidek, Fremont, California, USA) before cycloplegia.The axial length (AL) was measured with IOL Master 700 (Carl Zeiss Meditec, Dublin, CA, USA).Cycloplegic refraction was performed using computer automatic optometry (KR-8900;Topcon, Tokyo, Japan) 20min after the cyclopentolate drops was used (1%; Alcon, Fort Worth, TX, USA).Swept sourceoptical coherence tomography (model DRI OCT Triton,Topcon, Tokyo, Japan) with a resolution of 1024 A scan/6 mm was used to measure the thickness of retinal layers with the center of macular.A radial scan with 12 lines centered on the fovea and separated by 30° was used to capture images.Built-in software was used to segment the layers and construct topographic maps.The average thickness of the retinal layers within 6-mm-diameter circle centered in the fovea was calculated automatically.
DNA Isolations and Bisulfite TreatmentGenomic DNA was extracted from peripheral blood samples using DNeasy Blood & Tissue Kit (Qiagen 69506, Germany) according to its protocol.Afterwards, DNA was quantified by a Qubit 3.0 Fluorometer (ThermoFisher) and stored at -20℃.DNA 500 ng of each sample was used to bisulfite converted using EZ DNA Methylation Kits (Zymo Research, USA).
Infinium Human MethylationEPIC 850K BeadChip Assay(Illumina 850K)The Infinium MethylationEPIC 850K BeadChip assay (Illumina) was performed in accordance with Illumina’s standard protocol.Bisulfite-converted DNA was amplified followed by enzymatic end-point fragmentation,precipitation and resuspension.Sample labeling, hybridization to chips and image scanning were performed and all 40 samples were processed on the same chipset to avoid a batch effect.No less than 10 biological repeats were conducted in each group.
Methylation Validation by PyrosequencingPCR amplification of bisulfite-treated DNA was performed with primers designed using PyroMark Assay Design Software 2.0.Pyrosequencing was performed in accordance with the manufacturer’s protocol on a PyroMark Q96 ID System(Qiagen).The Pyro Q-CPG software of the pyrosequencing device was used to automatically analyze the methylation status of each site.The sequences of the primers used for the four genes are listed in Table 1.
Data AnalysisStatistical analyses were performed using R software (version 2.1.1).βvalue was used to represent DNA methylation level.The CpG sites with |Δβ|>0.1 andP-value <0.05 in the case and control groups were considered significant.Student’st-test was used to compare differences in methylation levels and other parameters between the case and control groups.Chi-square test was used to compare categorical variables.Data were presented as mean±standard deviation for continuous variables, and as rates (proportions)for the categorical data.only the left eye parameters were used for statistical purpose.RawP-value was adjusted using Benjamini method (R 4.0.0P.adjust function with method=‘fdr’) to control false discovery rate.P<0.05 was considered statistical significance.Gene Ontology (GO) and the Kyoto Encyclopedia of Genes and Genomes (KEGG)pathway enrichment analysis were performed using the scripts in Python to clarify the function and biological pathways of discovered DMS (P<0.05).
RESULTS
Characteristics of ParticipantsThe first survey was conducted in 2019, and a total of 40 T1DM children was included.Since none of these participants had DR, we set the lowest 25% participants (10/40) with the thinnest mean macular retinal thickness as the case group, and the rest as the control group.Table 2 listed the clinical characteristics of the participants from this first survey.There was no difference in age, gender, T1DM duration, BMI, HbA1c, triglycerides,total cholesterol, AL and spherical equivalent refraction (SER)between the case and control groups.The Infinium Human MethylationEPIC 850K BeadChip assay was used to analyze and to compare the genomic DNA methylation patterns between the case and control groups of this survey.
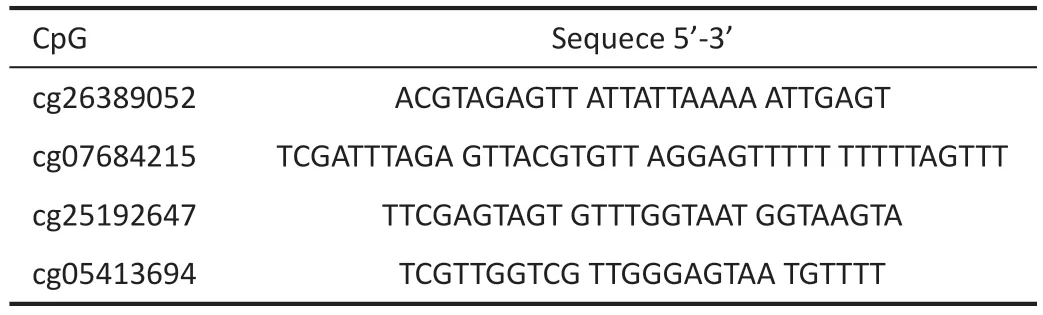
Table 1 Pyrosequencing primer sequences used in this study
The second survey was conducted in 2021.A total of 27 T1DM children was included, and four of them had DR.For these four participants with DR, only retinal microaneurysms were observed.Thus, we set these four DR patients as the case group, and the rest as the control group.The clinical characteristics of these 27 participants is listed in Table 2,and there was no difference in age, gender, T1DM duration,BMI, HbA1c, triglycerides, total cholesterol, AL and SER between the case and control groups.For this second survey,pyrosequencing assay was used to further investigate the results of the 850K BeadChip array from the first survey.
Quality Control of the 850K BeadChip Array DataGenome-wide DNA methylation profiles of the 40 participants from the first survey were generated using the Illumina Human Methylation EPIC 850 BeadChip.The density distribution and the boxplots of theβ-values were shown in Figure 1,which suggested that the overall distribution and concentration trend of the data in case group and control group were in a homogeneous distribution.
Comparison of the Genomic DNA Methylation Patterns Between Case and Control Groups Using the 850K BeadChip ArrayThe 850K BeadChip analysis revealed that 751 sites were significantly and differentially methylated in the case group when compared with the controls (|Δβ|>0.1 and Adj.P<0.05), while 328 of these were identified with a significance of Adj.P<0.01.Among these, 319 CpG sites were hypermethylated and 432 were hypometh ylated in the case group relative to the control group.A volcano plot and a heat map were used to present the differentially methylated CpG sites between the case group and the control group (Figure 2A,2B).The scatter plot of the average DNA methylation levels in the case group compared with those in the control group was presented in Figure 2C, with 432 hypomethylated sites and 319 hypermethylated sites shown in red.And the chromosomal distribution of the DMS were presented in Figure 2D, with the red denotes hypermethylated sites, and the blue denotes hypomethylated sites.

Figure 1 The distribution and concentration trend of the DNA methylation status A: The density distribution of the β-values in the case and control groups; B: The boxplots of the β-values distribution of the participants.

Table 2 The demographic systematic and ophthalmologic characteristics of the participated children from the first and the second surveys
GO functional enrichment and KEGG signaling pathway analysis were used to further investigate the signaling pathways associated with the DMS between the case and control groups to interrogate their biological functions.According to the criteria ofP<0.05 and false discovery rate <0.05, the top 30 most significant major signaling pathways were identified(Figure 3A, 3B).
Validating the Results of the 850K BeadChip Array by the Pyrosequencing AssayWe selected the Pyridoxal Kinase(PDXK, cg26389052), the Parkin RBR E3 Ubiquitin Protein Ligase (PRKN, cg25192647), the peroxisome proliferatoractivated receptor-gamma (PPARG, cg05413694) and the transcription elongation regulator 1 like (TCERG1L,cg07684215) genes to further investigate the methylation status by pyrosequencing.Our selection was based on two reasons: first, the 850K array indicated that these four genes were significantly and differentially methylated between the case and control groups of the first survey, suggesting that they are associated with macular retina thinning, which is assumed as an early sign of T1DM related retinal damage before the onset of DR; second, former studies indicated that these four genes has a potential role in diabetes[20-22].The most significant site is selected if multiple CpG sites are mapped to the same gene.Pyrosequencing revealed that only theTCERG1L(cg07684215) gene (P=0.018) was hypermethylated in the four T1DM children with DR, which was consistent with the result from the BeadChip analysis.ThePDXK(cg26389052),PRKN(cg25192647) andPPARG(cg05413694) genes showed no difference (allP>0.05) in the methylation status between the case and control groups of the second survey (Figure 4).
DISCUSSION
In this study, we first used the 850K BeadChip array to screen for DMS related with retina thinning, which we hypothesized as a biomarker for early retinal damage before the onset of DR in T1DM children.Then, the pyrosequencing assay was used to further investigate whether or not the DMS identified by 850K BeadChip were associated with DR development in T1DM children.And our results indicated that theTCERG1Lgene (cg07684215) is more hypermethylated both in the non-DR T1DM children with retinal thinning, and in the T1DM children with DR compared, with the controls.
So far, only two former studies have discussed DNA methylation changes associated with DR development in T1DM patients.Agardhet al[8]conducted a genome-wide analysis study in 58 T1DM adults, and identified differential DNA methylation of 349 CpG sites (representing 233 genes)in cases with proliferative DR compared with controls with no/mild DR.Chenet al[7]discovered 153 hypomethylated loci and 225 hypermethylated loci in cases with progressed retinopathy or macroalbuminuria comparing to controls without complication progression in 63 T1DM adults using Infinium Human Methylation 450 Bead Chip Arrays.The study design and study population of these two studies are different from our research, and theTCERG1Lgene was not identified by these two studies.

Figure 2 The DNA methylation pattern of the case group compared with the control group A: The volcano plot showing the hypomethylated genes (blue) and the hypermethylated genes (red) differentially methylated between the case and the control groups; B: Heat map showing the differentially methylated CpG sites (blue, CpGs with the lowest methylation levels; red, CpGs with the highest methylation levels) between the cases and the controls; C: Scatter plot showing the average DNA methylation level in the case group compared with those in the control group.The 319 hypermethylated sites and 432 hypometh ylated are shown in red.D: The chromosomal distribution of differently methylated sites between the case and control groups (red denotes hypermethylated sites; blue denotes hypomethylated sites).

Figure 3 Gene Ontology (GO) functional enrichment and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway analysis results A: The top 30 functions from GO functional enrichment analysis; B: The top 30 pathways from KEGG pathway analysis.
cg07684215 is located within the body of theTCERG1Lgene at chr10:131092391-131311721 (hg38).As a paralog ofTCERG1, theTCERG1Lgene is a transcription elongation regulator that has been described to be involved in the pathogenesis of cancer and non-cancer-related diseases,including inflammatory bowel disease and colon cancer,suggesting that TCERG1L influences immunological pathways[23-25].Moreover, previous genome-wide association studies have found thatTCERG1Lis associated with insulin resistance and type 2 diabetes in African Americans, West Africans and individuals of Indian ancestry[26-27].Although T1DM belongs to chronic autoimmune disorders, as T-lymphocytes are activated to attack pancreatic β-cells[28],TCERG1Lhas not been reported previously to be associated with T1DM or DR.

Figure 4 Using direct bisulfite pyrosequencing to investigate the DNA methylation patterns of four genes previously identified by the 850K BeadChip Type 1 diabetic children with retinopathy were set as case group, and those without retinopathy were set as control.A: Methylation level of cg26389052 (pyridoxal kinase, PDXK); B: Methylation level of cg07684215 (transcription elongation regulator 1 like, TCERG1L); C:Methylation level of cg25192647 (parkin RBR E3 ubiquitin protein ligase, PRKN); D: Methylation level of cg05413694 (peroxisome proliferatoractivated receptor-gamma, PPARG).
We did not find any association between DR and the methylation status of thePDXK,PRKN,andPPARGgenes by the pyrosequencing assay.This inconsistency between the results of the 850K BeadChip array and the pyrosequencing assay is not unpredicted.The most probable reason of the inconsistency is the different grouping methods we used in the two surveys.As explained earlier, because none of the participants had DR in the first survey, we set the lowest 25% participants (10/40) with the thinnest mean macular retina thickness as the case group.This grouping method is based on the hypothesis that macular retina thinning could be used as a biomarker for T1DM related early retinal damage before the onset of DR.Although the hypothesis is supported by some former published researches[12-15]and our previous findings, macular retina thinning certainly does not equal to DR development.Other possible reasons for this inconsistency are mainly caused by the limitation of genome-wide DNA methylation tests, because DNA methylation variability can be composed of both biological and technical sources[29].
This study has several limitations.First, the number of the participants was small.Although we included totally 67 participants in the two surveys, which is comparable with the former T1DM studies[7-8], only 4 of them had DR.Because of the shorter disease duration, the prevalence of DR in T1DM children is significantly lower than that in the adults[30].Small case group may affect the result.We will repeat and improve the study once more T1DM children with DR appear.Second,conclusions of this study may only apply to Chinese children with T1DM.Future studies analyzing the association betweenTCERG1Land DR in T1DM patients with a larger case group and a different study population may reveal further evidences.In conclusion, our results reveals that the hypermethylation of theTCERG1Lgene is a risk factor for DR development in Chinese children with T1DM.This study is the first to report the relation between DR and DNA methylation changes in T1DM children, and may provide reference for the prevention,screening and early treatment of DR in T1DM patients.
ACKNOWLEDGEMENTS
Foundations:Supported by the National Key Research and Development Program of China (No.2016YFC0904800);National Natural Science Foundation of China (No.82101181);China Scholarship Council (No.201506230096); Shanghai Sailing Program (No.19YF1439700).
Conflicts of Interest: Qian Y,None;Xiao Y,None;Lin QR,None;Xiang ZY,None;Cui LP,None;Sun JQ,None;Li SC,None;Qin XR,None;Zou HD,None;Yang CH,None;Jin PY,None.
 International Journal of Ophthalmology2024年3期
International Journal of Ophthalmology2024年3期
- International Journal of Ophthalmology的其它文章
- Meibomian glands segmentation in infrared images with limited annotation
- Artificial intelligence for the detection of glaucoma with SD-OCT images: a systematic review and Meta-analysis
- Overexpression of TRPV1 activates autophagy in human lens epithelial cells under hyperosmotic stress through Ca2+-dependent AMPK/mTOR pathway
- Dry environment on the expression of lacrimal gland S100A9, Anxa1, and Clu in rats via proteomics
- Semaphorin 7A impairs barrier function in cultured human corneal epithelial cells in a manner dependent on nuclear factor-kappa B
- Novel MIP gene mutation causes autosomal-dominant congenital cataract