
Frequency and barriers of reporting workplace violence in nurses:An online survey in China
2021-02-28 09:48ChunynSongGiliWngHongynWu
Chunyn Song ,Gili Wng ,Hongyn Wu ,*
a Department of Nursing,Union Hospital,Tongji Medical College,Huazhong University of Science and Technology,Wuhan,Hubei,China
b Department of Cardiac Surgery,Union Hospital,Tongji Medical College,Huazhong University of Science and Technology,Wuhan,Hubei,China
Keywords:Hospital nursing staff Self report Violence Workplace
ABSTRACT Objectives:This study aimed to explore the reporting of workplace violence against nurses and the reasons why they did not reported.Methods:A self-designed questionnaire regarding workplace violence and reporting was used to conduct a cross-sectional survey on nurses who submitted a manuscript to a Chinese nursing journal from 2016 to 2017.A total of 324 nurses agreed to participate in this study and 266 participants from 165 hospitals in 72 cities returned questionnaires.Results:A total of 172 nurses (64.7%) experienced violent incidents during the past year.Of these incidents,45.5%were reported;and the reporting rate of physical assaults(69.0%)was higher than those of verbal abuse (36.9%),threatening behavior (51.7%),and sexual harassment (60.0%).Formal reporting accounted for 25.4% (15.4% in written form and 10.0% through a computer-assisted reporting system).Almost half of the nurses(49.6%)stated that the hospital had no reporting system or they were uncertain about the reporting system.For reasons of not reporting,51.9% of the nurses were unware of how and what types of violence to report,and 50.6%of the nurses believed that the hospital paid greater attention to patients rather than staff.Conclusions:A clear definition of workplace violence and reporting procedures,establishment of a facile system for reporting,and supervisory support following a reporting are urgently required.
What is known?
·Nurses are at high risk of becoming a target of workplace violence.
·Workplace violence affects individual physical and mental wellbeing,and in consequence,organizational problems.
·Under-reporting workplace violence is a worldwide phenomenon in the nursing profession.
·The reasons why nurses do not report violent incidents are not thoroughly studied and vary in different countries.
What is new?
·The majority of nurses participating in the survey tended to not report the workplace violence they experienced.Among those reported incidents,the reporting rate of physical assaults were higher than those of verbal abuse,threatening behavior,and sexual harassment.
·The most significant reasons for not reporting workplace violence included that nurses were unaware of how and what types of violence to report,followed by that hospitals usually paid greater attention to patients rather than to nursing staff,and the lack of supervisory support after reporting.Lack of a reporting system in hospitals may also be a potential cause.
1.Introduction
Workplace violence (WPV) against nurses is a global issue and has attracted increasing research attention.International literature agrees that nurses are at high risk of experiencing WPV,given their frontline position in the health-care system and the feminization of the nursing profession.The magnitude of nurses’exposure to WPV varies by countries and different settings are used for study designs and questionnaires.Thus,Spector et al.[1]carried out a quantitative review of 136 articles involving 151,347 nurses from 160 samples and reported that the overall violence exposure rates were 36.4% for physical violence,66.9% for nonphysical violence,39.7%for bullying,and 25% for sexual harassment.However,the review did not include Chinese researchs.In China,the prevalent and alarming violence directed at nurses has attracted recent research focus.In Shenzhen,a large city in Southern China,more than 10%of nurses had frequent experiences of WPV and 64.22%had occasional encounters[2].In another study on seven hospitals in Heilongjiang,a province in northeast China,7.8% of nurses had physical violent experiences and 71.9%had non-physical violent experiences[3].Shi et al.[4]conducted a cross-sectional survey in 44 tertiary hospitals and 90 county-level hospitals in 16 provinces (municipalities or autonomous regions)and found a 65.8%prevalence of WPV against Chinese nurses.Parallel to the high prevalence of WPV in nursing practice,exposure to violence has far-reaching consequences.Violent experience has negative effects on both nurses and the healthcare systems,especially in developing countries [5].These effects include deteriorated sub-health status,increased depressive symptom and work-related stress,and decreased organizational commitment,job satisfaction,and quality of work-life [6-11].
Despite the high prevalence of WPV encountered among nurses,under-reporting is a worldwide phenomenon in the nursing profession [12-14].A survey in Slovenia concluded that nurses reported violent incidents in formal written form ranging from 6.5%(psychological violence) to 10.9% (physical violence) [15].In another research[13],74.7%of nurses had been subjected to WPV,whereas only 18.2% formally reported all incidents and 15.6% reported none.The same tendency was found in Israel,where nearly 72% of nurses had experienced violent incidents,but only 26.6%filed reports in written form [14].Under-reporting impedes violence prevention efforts in two ways.First,under-reporting might lead to underestimation of the true extent of the problem,thus indicating less need for prevention of possible negative effects than may be warranted.Second,without knowledge of the full spectrum of violent incidents,prevention efforts can only be designed to affect its limited aspects [16].
Causes of under-reporting are complex and have not been thoroughly studied [17].Foreign studies have offered reasons or explanations for under-reporting.Nurses may not report if they perceive the aggressive behavior to be unintentional,that is,related to patient illness such as dementia,confusion,or disorientation[12,16,17].Nurses also feel reluctant to report incidents that may not be sufficiently serious or have a mild impact [17,18],for example,non-physical violence is reported less often than physical violence [18,19].Nurses were more likely to report if they were injured or lost time from work [16].One of the most significant reasons for not reporting was that nurses perceive violence as‘part of the job’ [12,18,20,21],that is,as their exposure to violence increases,the probability of reporting decreases because they believe WPV is routine or the norm.Another common reason for underreporting is the nurses’ belief that reporting would not lead to any positive changes,such as no preventative measures after the violent incident [12,15,18,20].Lack of awareness of reporting methods and mechanisms may be a possible cause of underreporting [12,22].Other barriers to reporting include the lack of clear policies and procedures [18]and nurses’ perception of timeconsuming reporting procedures [12,18].Other reasons for underreporting include lack of supervisory or coworker support,fear of blame,fear of losing one’s job,no encouragement to report,and heavy workload [12,18,23,24].The lack of a uniformly accepted definition of violence can also affect reporting behavior[16,17],and nurses may not define violent incidents as such if no physical injury was sustained [18].Socio-demographic factors such as gender,work experience,years of employment,childhood socialization,personal experience,and area of practice are also implicated as factors of reporting behavior [14,17,23].However,reporting WPV against nurses in China and the causes and barriers of underreporting have not been thoroughly examined.This issue needs clarification to develop strategies for reducing under-reporting and preventing WPV.
The current study aims to examine the magnitude and nature of reporting WPV in China and to identify reasons why victims do not report these incidents.
2.Methods
2.1.Study design and sample
An online cross-sectional survey was carried out using the Wenjuanxing Survey Tool.Potential participants were selected from authors who submitted a manuscript to a Chinese nursing journal from March 2016 to March 2017.Registered nurses who provide front-line care for patients for at least one year were included while those who had maternity or sick leaves in the past 12 months were excluded.
2.2.Survey instrument
The survey instrument measured nurses’ experience and reporting of WPV during the past year.The questionnaire included three parts.First,socio-demographic data included gender,age,education,department,employment nature,marital status,professional title,position,work year,the city where the hospital is located,hospital grade,and hospital type.The second part was the WPV experience and reporting.According to the International Labor Organization [25]and several studies,violence was defined as patient and visitor violence and classified into verbal abuse,threatening behavior,physical assault,and sexual violence[14,26,27].Examples of each type of violence were given.Verbal abuse is defined as offensive words that humiliate,degrade,or otherwise indicate a lack of respect for the dignity and worth of an individual.Threatening behaviors are warnings of intent to injure another person with or without an object or weapon.Physical assault includes slapping,pinching,pushing,shoving,spitting,or kicking,with or without weapons,and is subdivided into four levels:1) physical assault without body injury; 2) physical assault causing mild injuries,such as pain,scratches,swelling,and bruises;3) physical assault causing apparent injuries,such as wounds,fracture,and visceral or brain injury;and 4)physical assault causing severe injuries,such as functional disorder or disability.Sexual violence is any unwanted,unreciprocated,or unwelcome behavior of a sexual nature that is offensive to the person involved and that causes that person to feel threatened,humiliated,or embarrassed.This type includes verbal or non-verbal sexual harassment,sexist jokes,sexual innuendo,unnecessary touching,fondling,forced sexual intercourse,and attempted rape or rape.Nurses were asked whether they experienced WPV during the past 12 months and whether they had reported the violent incidents to their supervisors.Response alternatives of WPV experience were “No,never,”“Yes,once,” “Yes,twice or triple,” and “Yes,several times”; and response answers of reporting were “Yes” or “No”.The third part included three more questions on reporting:whether the hospital had a WPV reporting system;how WPV was reported (verbally,in written form,or through the computer system);and reasons for not reporting WPV (14 options,multiple-choice question).We invited 10 healthcare-related experts to evaluate the content validity and 20 nurses to verify the test-retest reliability of the questionnaire.The content validity index was 0.906 and the two-week test-retest reliability was 0.931.
2.3.Data collection
The e-mail contacts of the authors were exported to Microsoft Excel 2007 and then 1,100 subjects were randomly selected.An invitation letter was sent via e-mail,and those who agreed to participate were provided with a link to the survey using the Wenjuanxing Survey Tool.All participants were twice informed of the purpose of this study through the invitation letter and the questionnaire.Participants voluntarily and anonymously completed the questionnaire.In total,1,013 e-mails were successfully sent and 87 e-mail addresses were invalid.Among the respondents,324 agreed to participate and 266 questionnaires were returned and deemed valid for statistical analysis.
2.4.Ethical consideration
This study was approved by the Research Ethics Committee of our academic institution (IORG No:IORG0003571).Before the survey,all participants were well informed of the study details,including the preservation of confidentiality and anonymity (no personal name was required),purpose,inclusion criteria,and voluntary participation.During the survey,the study purpose and participant anonymity were reinforced,and participants could opt to reject the survey.
2.5.Data Analysis
The Statistical Package for Social Sciences Version 13.0 for windows (SPSS Inc.,Chicago,IL) was used for data analysis.Basic descriptive analysis was carried out on participants’ sociodemographic characteristics,reporting status,reporting methods,reporting system,and reasons for not reporting.
3.Results
3.1.Participant characteristics
Among the participants,only three were males and the other 263 were females.Most (237,89.5%) were married.Most nurses(77.4%) were in the institutional system and 64.7% worked in the medical/surgical ward (Table 1).The 266 respondents worked in 165 hospitals located in 72 cities of 27 provinces in China.The settings were mainly tertiary level (88.5%) and general (77.8%)hospitals.
3.2.Reporting status
Of the 266 nurses surveyed,172(64.7%)had experienced at least one type of violent incidents within the past 12 months.The total counts of different type of violent events encountered was 286,of which 130(45.5%)were reported and 156(54.5%)were not.For the types of WPV,verbal abuse had an incidence rate of 60.2% and a reporting rate of 36.9%;threatening behavior had an incidence rate of 32.7% with a reporting rate of 51.7%; physical assault had an incidence rate of 10.9% with a reporting rate of 69.0%,and sexual harassment had an incidence rate of 3.8% with a reporting rate of 60.0%.Table 2 shows the WVP types and reporting status.
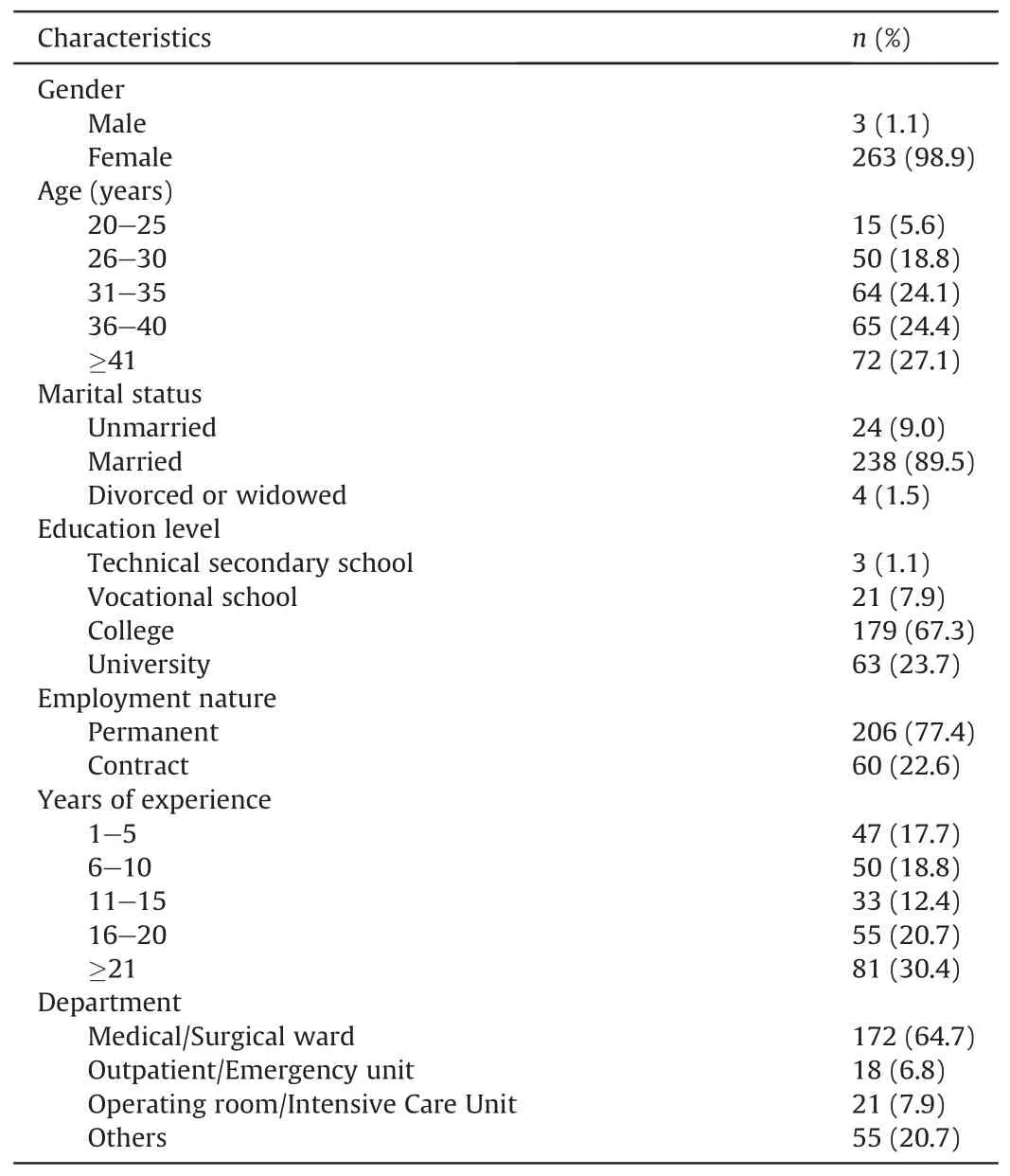
Table 1 Demographic information of participants (n=266).
3.3.Forms of reporting
Of the 130 reported violent incidents,97 (74.6%) were only verbally reported,20(15.4%)were reported in written form,and 13(10.0%) were reported through a computer system.
3.4.Reporting system
Of the total 266 respondents,134 (50.4%) stated that their hospitals had a WPV reporting system,62(23.3%)stated that their hospitals had no reporting system;and 70(26.3%)stated that they did not know whether or not their hospitals had a reporting system.
3.5.Reasons for not reporting
More than half of the nurses (51.9%) were unaware of how and what types of violence to report,followed by hospitals that paid more attention to patients rather than medical staff(50.6%),and no support and attention from the hospital (38.5%) after reporting.Table 3 shows the reasons for not reporting WPV.
4.Discussion
4.1.Verbal abuse was the most frequent form of violence
This study not only explores the reporting status of WPV encountered by nurses in China but also identifies the barriers to such reporting.As hypothesized,the results showed that the majority of nurses (64.7%) had experienced WPV in the proceeding year.Verbal abuse was the most frequent form of violence,followed by threatening behavior,physical violence,and then sexual violence.The results were similar to the recent quantitative reviewof 136 articles related to violence against nurses[1]and Jiao’s study in Heilongjiang province in China[3].Further comparisons with the other researchs were excluded given that the focus of the present study was to determine the magnitude and reasons for underreporting WPV among nurses.

Table 2 Frequency of nursing workplace violence over the past year among participants [n (%)].
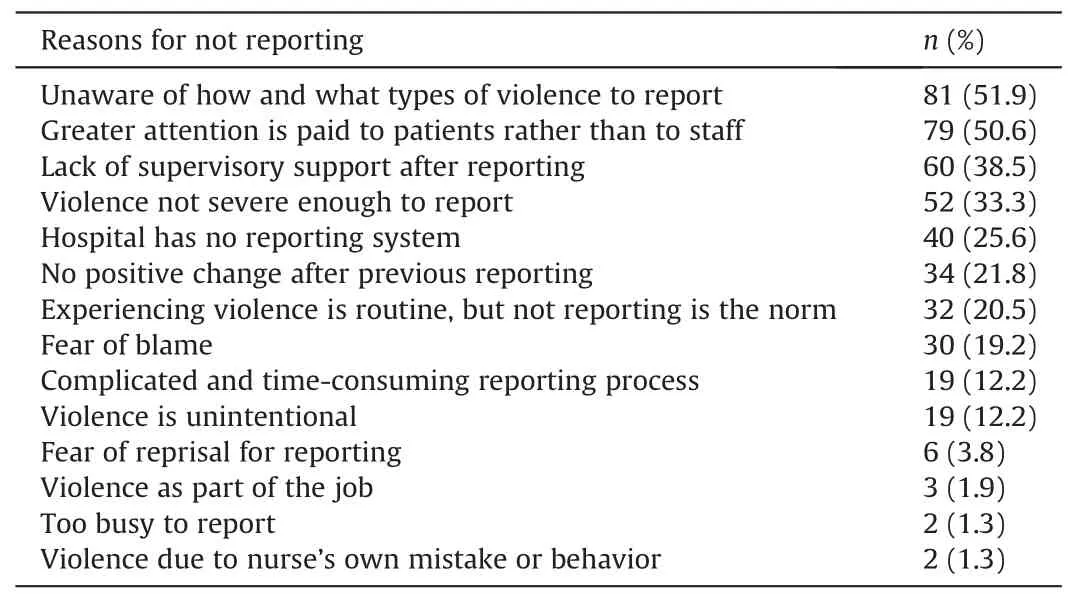
Table 3 Reasons for not reporting workplace violence among participants (n=156).
4.2.Under-reporting of violence is a significant problem in the nursing profession
This study confirmed that under-reporting of violence is a significant problem in the nursing profession.Of the violent incidents that nurses experienced,only 45.5% were reported,indicating a severe under-reporting.The reporting rate of WPV among Israeli nurses was 69.6%[14].Kvas and Seljak[15]found that 41.7%-50.9%of nurses in Slovenia reported WPV to superiors or professional association/union.Findorff et al.[19]also stated that 57%and 40%of physical and non-physical WPV,respectively,were reported to employers.The under-reporting phenomenon in China may result from a lack of reporting mechanisms.Almost half of the nurses(49.6%)stated that their hospital did not have a reporting system or uncertain of such a process.The findings indicate that the top management of these hospitals needs to establish a system for enabling and encouraging WPV reporting.Secondly,positive reporting culture encourages reporting.Reporting violence perpetrated against nurses in the workplace is required by Israel’s Ministry of Health,and the Nurses and Midwives Association and Union of Nurses in Slovenia have formulated action protocols for violent incidents and help its members to take appropriate actions following such events.These measures may provide the enlightenment that zero-tolerance to violence policy and practical guidance support reporting.The government can also implement a zero-tolerance policy and encourage reporting of violence,and thereby diminish or prevent WPV.Moreover,authoritative scholar associations can design guidelines for the prevention of and actions following violent incidents.
4.3.Verbal reports of workplace violence are more than written reports
This study revealed that violent incidents were more often reported verbally (74.6%) than in written form (15.4%) or through a computer reporting system(10.0%).This result corresponds with a study in Israel where verbal reporting was the most prevalent form(96.2%)and written reporting was 26.6%[14].The possible reason is that verbal reporting is easier,more easily available,and takes less time than written reports.However,Arnetz et al.[16]claimed that verbal reporting may not always be available to upper management for policy decisions,and therefore formally documented reporting is required to provide accurate data.Kvas and Seljak also advocated written reporting according to the protocol [15].However,formal reporting completed either in written form or through an electronic reporting system was not satisfactorily implemented with only a range from 6.5% to 12% [15,16].The results also show a relatively low share of WPV victims with informal reporting.Managers should take appropriate measures to enhance the formal reporting of WPV.Stene et al.[21]designed a paper-version reporting tool,which identifies the patient name,medical record number,incident date,and a brief description of the incident,taking approximately 1-2 min to complete the reporting.Henceforth,the reporting rate significantly improved.Considering the disadvantages of the paperversion reporting system,such as missing data,a time-consuming process,and errors in coding or entering data into the database,a simplified electronic reporting system may be urgently needed.
4.4.Reasons for the low rate of reporting violent incidents are complex
The results state that the most important reason for not reporting was that nurses were unaware of how and what types of violence to report.These findings were parallel to a recent Indian study that the low rate of reporting is due to a lack of awareness about the reporting mechanism of WPV [22],but not to the aforementioned studies in Israel and Slovenia [14,15].Kvas and Seljak found that the main reason for not reporting WPV was the belief that reporting would not change anything,followed by the fear of losing one’s job [15],while Natan et al.[14]stated that nurses’ normative beliefs regarding reporting violence had the largest effect on the intention to report.The perception of the type and degree of violence and lack of awareness about reporting methods and mechanisms might influence the reporting of WPV to a certain extent[12,28].The second most significant barrier of not reporting was organizational culture and attitudes toward violence.Among the subjects,half (50.6%) stated that more attention was given to patients rather than to healthcare staff after reporting,38.5%were convinced of the lack of supervisory support,and 21.8%believed that reporting the event would not change anything.These results were consistent with those of other researchs,particularly the belief that reporting would not effect changes[13,15,20]and lack of supervisory or coworker support[17,20].Sato et al.[17]also demonstrated that managerial unwillingness to defend staff nurses from aggressive behavior was significantly associated with reporting behavior at all levels.A possible explanation for the results might be the avoidance of damaging the doctor-patient relationship in China [29].When violence occurs,the hospital immediately attempts to pacify the patient rather than support healthcare workers.Consequently,reporting with no responses might cause feelings of apathy among the victims and cultivate the notion that their reports would not be investigated appropriately [30],which would impede their future reporting.Therefore,managers need to establish a system of high organizational responsiveness to WPV[31].The present study also showed that 19.2% of the nurses feared being blamed after reporting,consistent with the results of other studies[17,20].Fortunately,the present study showed that only 1.9% of nurses who did not report WPV considered such incidents as part of the job,although this was previously found as an important cause of under-reporting[12,18,20,21].
Parallel to prior research,the present study found that reporting had a higher likelihood when the symptoms or effects of the violence were more severe [16,17,19].This finding may in part be explained by the fact that nurses injured in a violent incident might lose time from work to seek care.The other potential explanation is the nursing principles that emphasize caring and empathy,thus leading to a culture of tolerance and acceptance of violence.Nurses were more likely to endure rather than report verbal abuse,threatening behavior,or mild physical assault.Thus,reporting of mild incidents of WPV should be encouraged.To prevent a major injury,we should also analyze incidents that cause no injuries.
4.5.Limitation
Several limitations in this study require noting.First,participants are selected from authors of a Chinese journal,and thus selection bias may occur to a certain extent due to the scientific research ability and participants’ preference toward the journal.Second,a relatively low response rate might threaten the survey validity by increasing a non-response bias [32]because the population that did not participate was not represented.Third,due to the relatively small sample size,further analysis was not carried out to explore the relationships between reporting of WPV and sociodemographic characteristics.Such analysis can help to identify vulnerable groups of under-reporting.Fourth,retrospective data collection might depend on respondents’ memory of events that occurred within 12 months before the survey,potentially resulting in recall bias.Moreover,the use of self-report is another limiting factor because of the possible creation of biased answers resulting from the use of defense mechanisms or social desirability.Arnetz et al.[16]also found that 23%of respondents stated that they selfreported violent events,when in fact only 4% had done so.These limitations may prevent the generalization of the results in China,although the magnitude of underreporting might be valuable for arousing interest in this topic.
5.Conclusions
The research findings show that nearly two-thirds of participants experienced WPV,but only less than half of these incidents were reported.Verbal reporting was the predominant form while formal reporting was relatively low.Reporting behavior was found to be associated with the types of violence.Verbal abuse was reported less often than threatening behavior,physical assault,and sexual harassment.The most common reason for not reporting was that nurses were unaware of how and what types of violence to report,followed by the perceived lack of support from the hospital after a violent incident.The absence of a hospital reporting system might also be a potential barrier.
To increase the share of reported WPV,healthcare organizations or hospitals should clearly define violence to create uniform definitions of the term that contribute to nurses’ understanding of violence.The significance of reporting and the magnitude of underreporting should be discussed to encourage nurses’ willingness to participate in reporting and provide their opinions and suggestions for the prevention of under-reporting.Second,healthcare organizations or hospitals should define a clear and simple reporting mechanism to show nurses how and what to report.Formal reporting forms such as unified written or electronic reporting systems are required to improve the process.Difficult and timeconsuming use of the reporting system was a major barrier to reporting [18].Therefore,the reporting system must be quick and simple to use.Moreover,all employees must be acquainted with the reporting process and know how to report.Third,although important,the simplification of the reporting procedure would not suffice,and senior management support was necessary [12].Managers have a pivotal role in encouraging the reporting of violent incidents and should therefore change attitudes toward violence and treat it as unacceptable.When receiving a violent incident report,specific actions should be taken,such as following up individually with each victim to ensure his or her well-being,providing support to the person reporting to change the institutional culture,and establishing a follow-through with the institutional reporting [21].These measures might allow the victims to perceive that they are appropriately protected after submitting a report.An intervention study also confirmed that providing education,leadership support,and tool to report violent incidents reinforced the behavior of reporting in emergency department staff[21].Furthermore,Ferns et al.[12]recommended the development of autonomous practice and empower management to increase nurses’ self-value and confidence to report WPV.In summary,managers,educationalists,researchers,and individual nurses all have a role in encouraging the reporting of violent incidents.A comprehensive strategy should be taken to ensure that all incidents of violence are reported and assessed to provide credible data for minimizing WPV.
CRediT authorship contribution statement
Chunyan Song:Investigation,Formal analysis,Writing-Original draft.Gaili Wang:Investigation,Writing-Review and Editing.Hongyan Wu:Conceptualization,Methodology,Formal analysis.
Declaration of competing interest
The authors declare of no conflicts of interest.
Acknowledgment
We thank Ping Yin,Professor of Statistics,the Department of Statistics,Tongji Medical College,Huazhong University of Science and Technology (HUST) for assistance in statistical analysis.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2020.11.006.
 International Journal of Nursing Sciences2021年1期
International Journal of Nursing Sciences2021年1期
- International Journal of Nursing Sciences的其它文章
- Focuses and trends of the studies on pediatric palliative care:A bibliometric analysis from 2004 to 2018
- Relationship between negative emotions and perceived support among parents of hospitalized,critically ill children
- The effect of digital health technologies on managing symptoms across pediatric cancer continuum:A systematic review
- Effectiveness of animal-assisted therapy on pain in children:A systematic review and meta-analysis
- Effects of creative expression program on the event-related potential and task reaction time of elderly with mild cognitive impairment
- Struggling to live a new normal life among Chinese women after losing an only child:A qualitative study