
Clinical factors predicting rotavirus diarrhea in children:A crosssectional study from two hospitals
2023-12-25 00:55MichelleIndrawanJasonChendanaTanGabriellaHeidinaHandokoMelanieWidjajaGilbertSterlingOctavius
Michelle Indrawan,Jason Chendana,Tan Gabriella Heidina Handoko,Melanie Widjaja,Gilbert Sterling Octavius
Michelle Indrawan,Jason Chendana,Tan Gabriella Heidina Handoko,Melanie Widjaja,Gilbert Sterling Octavius,Department of Pediatric,Universitas Pelita Harapan,Banten 15811,Indonesia
Abstract BACKGROUND Rotavirus is still a significant contributing morbidity and mortality in pediatric patients.AIM To look at clinical signs and symptoms and laboratory findings that can predict rotavirus gastroenteritis compared to non-rotavirus gastroenteritis.METHODS This was a cross-sectional study with medical records obtained from December 2015 to December 2019.Inclusion criteria for this study include all hospitalised pediatric patients(0-18 years old)diagnosed with suspected rotavirus diarrhea.The receiver operating curve and Hosmer-Lemeshow test would be used to assess the final prediction findings' calibration(goodness of fit)and discrimination performance.RESULTS This study included 267 participants with 187(70%)rotavirus-diarrhea cases.The patients were primarily male in both rotavirus(65.2%)and non-rotavirus(62.5%)groups.The median age is 1.33 years old(0.08-17.67 years old).Multivariate analysis shows that wet season(ORadj = 2.5;95%CI:1.3-4.8,Padj = 0.006),length of stay(LOS)≥ 3 days(ORadj = 5.1;95%CI:1.4-4.8,Padj = 0.015),presence of abdominal pain(ORadj = 3.0;95%CI:1.3-6.8,Padj = 0.007),severe dehydration(ORadj = 2.9;95%CI:1.1-7.9,Padj = 0.034),abnormal white blood cell counts(ORadj = 2.8;95%CI:1.3-6.0,Padj = 0.006),abnormal random blood glucose(ORadj = 2.3;95%CI:1.2-4.4,Padj = 0.018)and presence of fecal leukocytes(ORadj = 4.1,95%CI:1.7-9.5,Padj = 0.001)are predictors of rotavirus diarrhea.The area under the curve for this model is 0.819(95%CI:0.746-0.878,P value < 0.001),which shows that this model has good discrimination.CONCLUSION Wet season,LOS ≥ 3 d,presence of abdominal pain,severe dehydration,abnormal white blood cell counts,abnormal random blood glucose,and presence of fecal leukocytes predict rotavirus diarrhea.
Key Words: Rotavirus;Pediatric;Gastroenteritis;Diarrhea;Indonesia
INTRODUCTION
Rotavirus gastroenteritis accounted for 19.11% of diarrheal deaths worldwide in 2019 and is still a leading cause of morbidity and mortality,especially in children under five.Surveillance data from 2008-2018 showed that 40.78% of all diarrheal diseases in children in Southeast Asia were attributable to rotavirus infection[1].The fecal-oral transmission from person-to-person contact or ingestion of fecally contaminated food and water commonly leads to a rapid spread among communities,especially in developing countries[2].
When diagnosing gastroenteritis,it is necessary to analyse fecal specimens using widely available assays because rotavirus-caused gastroenteritis cannot be clinically distinguished from that caused by other enteric pathogens[3].However,because the findings do not change clinical management,which primarily depends on effective rehydration therapy,rotavirus is not routinely tested for in patients with gastroenteritis[4].Despite its worldwide prevalence,detecting rotavirus in stool samples is still a logistical and financial challenge in developing countries[5].
Considering the disease burden,it is essential to know reliable clinical signs and symptoms and other nonconfirmatory laboratory tests that clinicians can use to guide their treatment.Hence,this study aims to look at clinical signs and symptoms and laboratory findings that can predict rotavirus gastroenteritis compared to non-rotavirus gastroenteritis.
MATERIALS AND METHODS
This study was cross-sectional,with medical records obtained from December 2015 to December 2019 from Siloam General Hospital and Siloam Hospital Lippo Village(SHLV).Patients covered by Indonesia's national health insurance can receive care at Siloam General Hospital,a teaching hospital.SHLV,on the other hand,primarily consists of patients who are self-paying or have private insurance.Inclusion criteria for this study include all hospitalised pediatric patients(0-18 years old)diagnosed with suspected rotavirus diarrhea,defined as the passing of ≥ 3 watery or loose stools each day[6].Children who have previously experienced significant immunosuppression due to prolonged steroid usage or illnesses like the human immunodeficiency virus or primary immunodeficiency were excluded from this study.Another exclusion criterion was the presence of concurrent infections such as urinary tract infections or pneumonia.The sample size calculation used the following formula:
Where N is the sample size,z denotes the standard error,which was 1.96,p was the estimated prevalence in the population,q was 100-p,and e was the acceptable sample error set at 6% in this study.The prevalence of pediatric rotavirus diarrhea in Indonesia is 37.5% to 53.5%[7].Hence,the minimum sample size required was 265 children.
We collected demographic data such as age,gender,and nutritional status.Clinical signs such as temperature upon arrival,vital signs,clinical manifestations(abdominal pain,respiratory symptoms,dehydration status according to World Health Organization(WHO)[6],duration and frequency of symptoms(diarrhea,vomiting,fever),length of stay(LOS),treatment given during hospitalisation [intravenous(IV)rehydration and any antibiotics],rotavirus vaccination status,as well as the seasons during which the children contracted diarrhea.The need for IV rehydration represented severe dehydration in this study.Meteorology Climatology and Geophysics Council's data in 2017 were used to determine the seasons where October-February was the rainy season,and the rest was the dry season in Tangerang[8].We adhered to WHO 2006 growth chart for children below five years,while the Centers for Disease Control and Prevention 2000 growth charts were used for children aged 5-18 years old to classify nutritional status[9].We did not collect any data on zinc used for diarrhea as all children were given zinc for diarrhea as per standard protocol in our hospitals.Lastly,we collected laboratory findings such as complete blood count,serum electrolytes,random blood glucose,erythrocyte sedimentation rate(ESR),and urinary ketone for dehydration markers and fecal leukocytes[10].We present laboratory values dichotomously(normalvsabnormal values)for multivariate analysis and in numerical forms for descriptive purposes.The reference range will be based on our population study's mean or median age group.
The neutrophil-lymphocyte ratio(NLR)is obtained by dividing the total band and segmented neutrophil by the lymphocyte.In contrast,the monocyte-lymphocyte ratio is obtained by dividing the monocyte by the lymphocyte.Absolute neutrophil count is calculated with the formula as follows:(Total WBC × % [PMNs + bands])÷ 100.
While the absolute lymphocyte count is calculated with the formula:WBC count × 1000 × % lymphocyte.(NLR were obtained by dividing the total neutrophils by lymphocyte counts,and the same methodology was applied to obtain lymphocyte-to-monocyte ratio(LMR)and platelet-to-lymphocyte ratio(PLR)[11].One or two ccs of peripheral venous blood samples were collected by antecubital venipuncture into vacutainer tubes(Becton Dickinson,Rutherford,NJ,United States)containing tri potassium ethylenediaminetetraacetic acid.The complete blood count was done within one to two hours after the blood samples were drawn,and the analysis was performed using the Advia 2120i automated analyser(Siemens Healthcare Diagnostics,Deerfield,IL,United States).Erythrocyte sedimentation rate levels were measured by TEST 1(Alifax,Padova,Italy).The rotavirus analysis was done using immunochromatography(Alcore One-Step Rotavirust Test).Those who tested positive would be categorised as having rotavirus diarrhea,and those who tested negative would be categorised as having non-rotavirus diarrhea.Strict quality control procedures were adopted.All of the independent variables were chosen based on previous studies[7,12,13].
The data was processed using IBM SPSS 26.0(Statistical Package for the Social Sciences,IBM Corp.,Armonk,NY,United States).After a normality test,data with a normal distribution will be presented as mean and standard deviation.If not,the median and range will be applied.The Mann-Whitney-U test is used when the distribution of numerical data is non-normal,while the T-test is used when the distribution of numerical data is normal.Chi-square was used for bivariate analysis,and variables with p-values less than 0.25 would be used in multivariate logistic regression analysis.The receiver operating curve(ROC)and Hosmer-Lemeshow test would be used to assess the final prediction findings' calibration(goodness of fit)and discrimination performance.The area under the curve(AUC)is equal to 0.5 when the ROC curve represents chance,and it is equal to 1.0 when the ROC curve represents accuracy.A good calibration would be indicated by aPvalue > 0.05.The sensitivity and specificity of the various predictor variables in identifying non-severe and severe pneumonia were then calculated using the area under the curve.We also analysed casewise diagnostics to identify any outliers.
This study protocol was approved by the Committee on Ethics at the University of Pelita Harapan,Tangerang,Indonesia,with Code Ethic No.430/FK-UPH/Ext./V/2019.The ethical board exempted informed consent due to the retrospective nature of our study.Identities were removed entirely,and data were analysed anonymously.
RESULTS
Descriptive characteristics
This study included 267 participants with 187(70%)rotavirus-diarrhea cases(Table 1).The patients were primarily male in both rotavirus(65.2%)and non-rotavirus(62.5%)groups.The median age is 1.33 years old(0.08-17.67 years old),with the majority belonging to the 0-11 mo old category(34.5%).Most patients had good nutritional status in the non-rotavirus group(51.3%)and rotavirus group(53.5%).Most rotavirus cases occurred during the dry season(77.1%),while nonrotavirus cases occurred mainly in the wet seasons(37.8%)with an odds ratio(OR)of 0.49 [95% confidence interval(CI)0.29-0.93,Pvalue 0.01].The majority of patients had a length of stay of ≥ 3 d in both groups(95% in the non-rotavirus group and 83.4% in the rotavirus group)(OR 0.27;95%CI:0.1-0.78,Pvalue 0.02).Only one patient was put in the intensive care unit,belonging to the non-rotavirus group.In both groups,most patients are not vaccinated for rotavirus(86.3% in non-rotavirus diarrheavs94.7% in rotavirus diarrhea)with an OR of 0.35(95%CI:0.14-0.97,Pvalue 0.04)(Table 1).
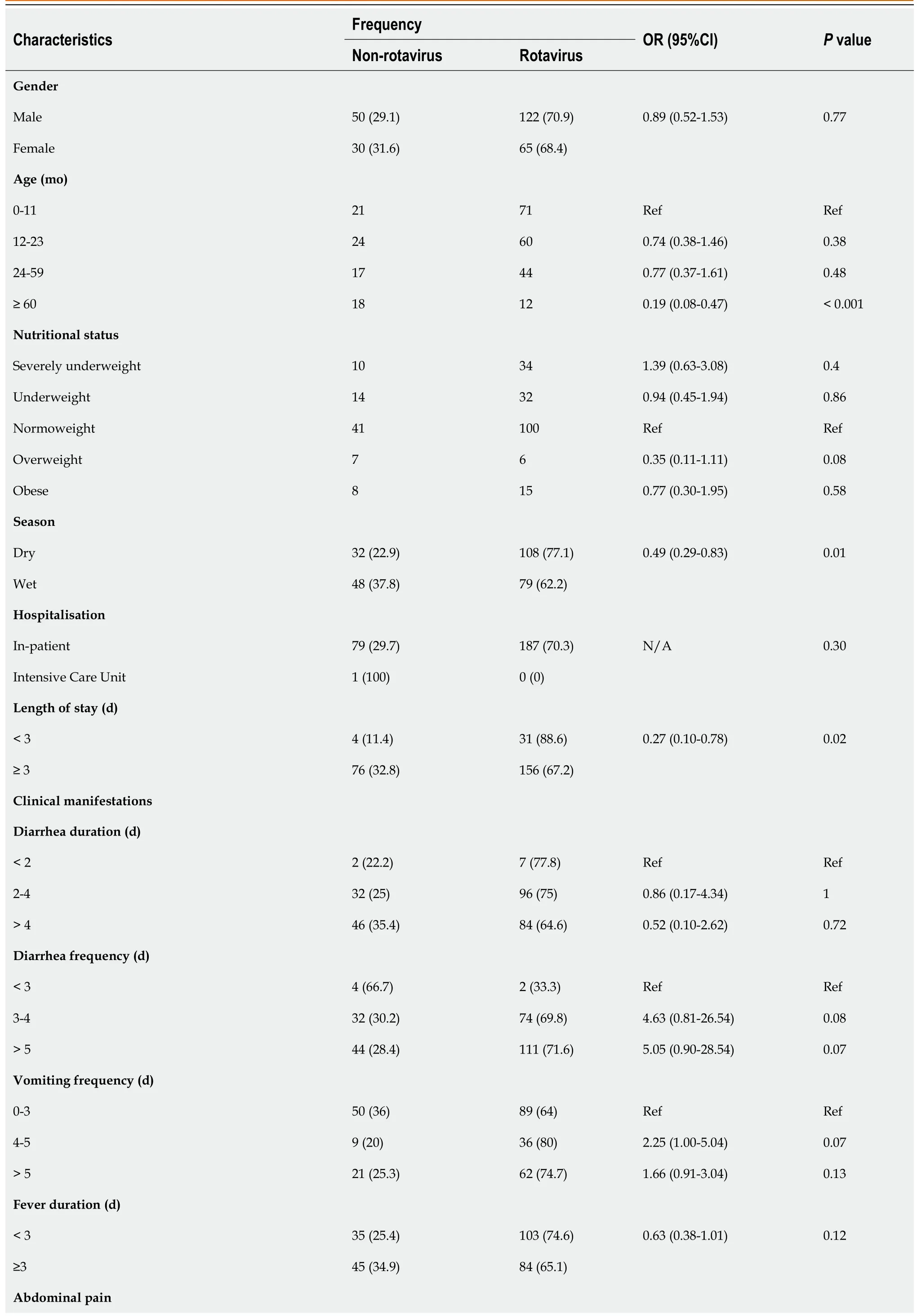
Table 1 Characteristics of the study population
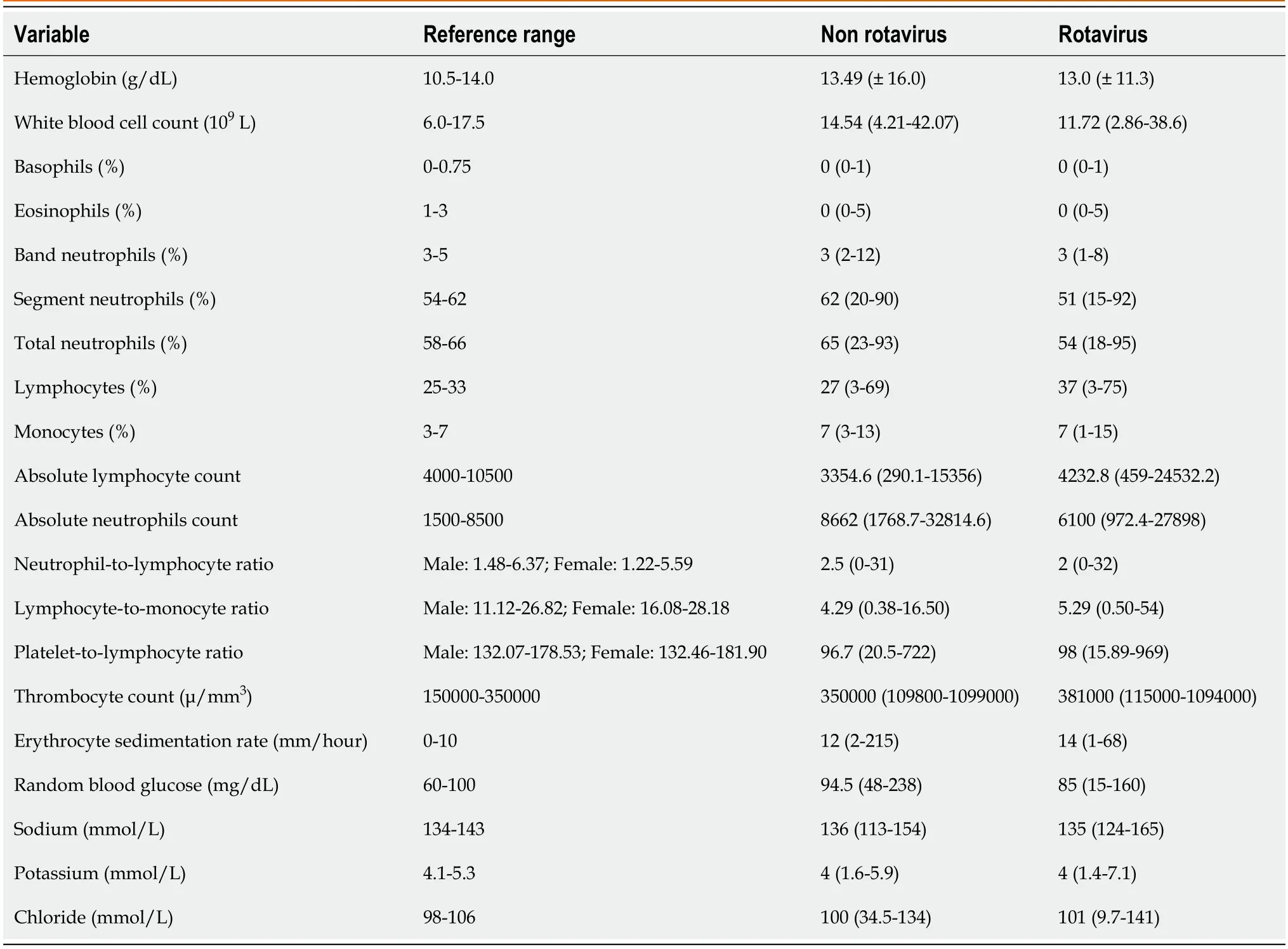
Table 2 Descriptive values of the laboratory findings
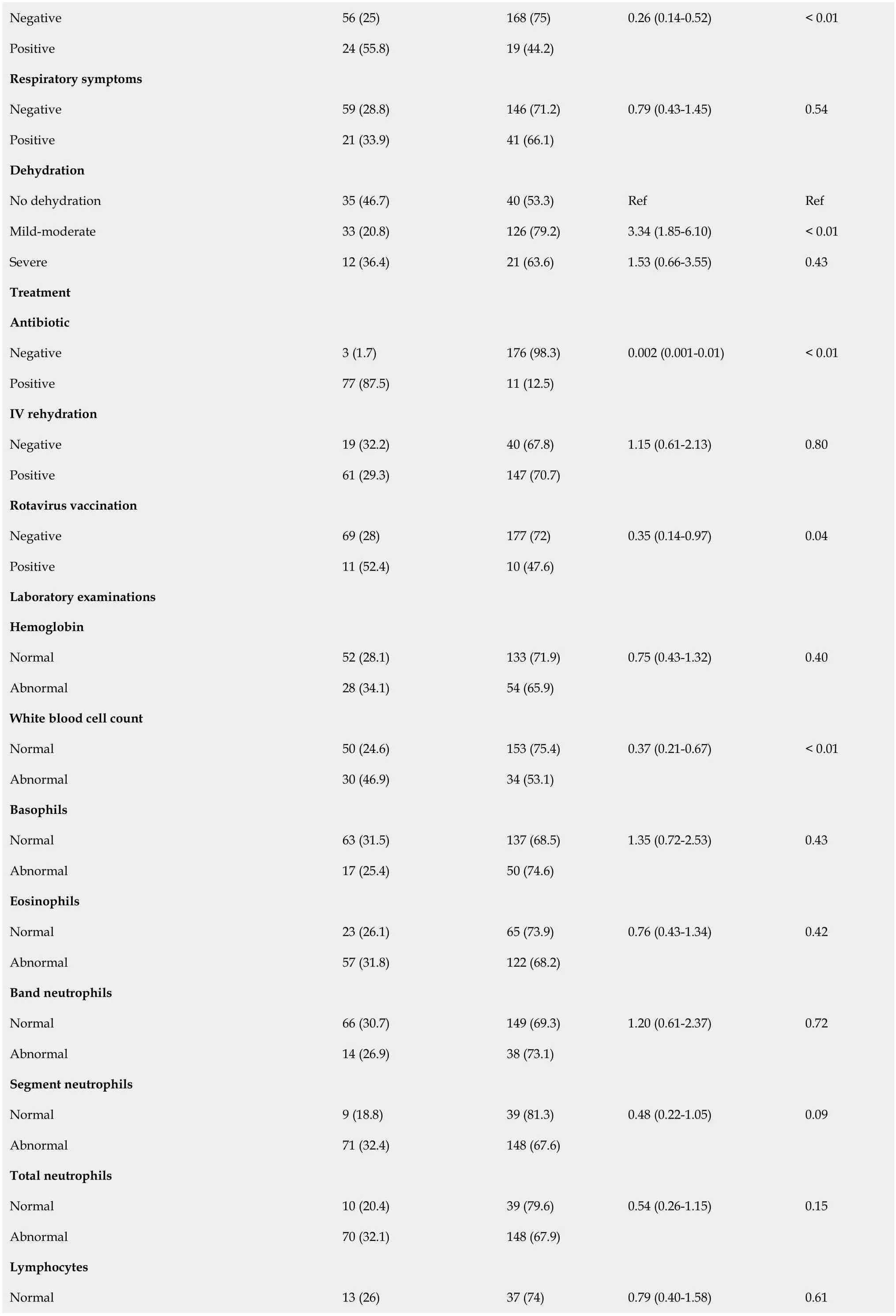
Negative 56(25)168(75)0.26(0.14-0.52)< 0.01 Positive 24(55.8)19(44.2)Respiratory symptoms Negative 59(28.8)146(71.2)0.79(0.43-1.45)0.54 Positive 21(33.9)41(66.1)Dehydration No dehydration 35(46.7)40(53.3)Ref Ref Mild-moderate 33(20.8)126(79.2)3.34(1.85-6.10)< 0.01 Severe 12(36.4)21(63.6)1.53(0.66-3.55)0.43 Treatment Antibiotic Negative 3(1.7)176(98.3)0.002(0.001-0.01)< 0.01 Positive 77(87.5)11(12.5)IV rehydration Negative 19(32.2)40(67.8)1.15(0.61-2.13)0.80 Positive 61(29.3)147(70.7)Rotavirus vaccination Negative 69(28)177(72)0.35(0.14-0.97)0.04 Positive 11(52.4)10(47.6)Laboratory examinations Hemoglobin Normal 52(28.1)133(71.9)0.75(0.43-1.32)0.40 Abnormal 28(34.1)54(65.9)White blood cell count Normal 50(24.6)153(75.4)0.37(0.21-0.67)< 0.01 Abnormal 30(46.9)34(53.1)Basophils Normal 63(31.5)137(68.5)1.35(0.72-2.53)0.43 Abnormal 17(25.4)50(74.6)Eosinophils Normal 23(26.1)65(73.9)0.76(0.43-1.34)0.42 Abnormal 57(31.8)122(68.2)Band neutrophils Normal 66(30.7)149(69.3)1.20(0.61-2.37)0.72 Abnormal 14(26.9)38(73.1)Segment neutrophils Normal 9(18.8)39(81.3)0.48(0.22-1.05)0.09 Abnormal 71(32.4)148(67.6)Total neutrophils Normal 10(20.4)39(79.6)0.54(0.26-1.15)0.15 Abnormal 70(32.1)148(67.9)Lymphocytes Normal 13(26)37(74)0.79(0.40-1.58)0.61

N/A:Not applicable.
Clinical manifestations
The clinical manifestations vary between the two groups.Most patients presented with mild-moderate dehydration(67.4%)in rotavirus diarrhea,while most in the non-rotavirus group presented with no dehydration(43.8%).Fever mostly lasts less than three days for rotavirus diarrhea(55.1%),while fever lasts mostly ≥ 3 d in the non-rotavirus group(56.3%).The last difference in clinical manifestation between the two groups is in diarrhea duration,where in rotavirus diarrhea it lasts 2-4 d(51.3%)while it mostly lasts > 4 d(57.5%)in the non-diarrhea group.Meanwhile,in both groups,most patients suffer from more than five diarrhea episodes per day,0-3 vomiting episodes,abdominal pain,and respiratory symptoms(Figure 1).

Figure 1 The receiver operating curve curve analysis.
Treatment
98 .3% of patients that are rotavirus positive did not receive antibiotics.In comparison,almost all(96.3%)patients who suffer from non-rotavirus diarrhea receive antibiotics with an OR of 0.002(95%CI:0.001-0.01,Pvalue < 0.01).In both groups,most patients receive IV rehydration with no significant statistical difference(OR 1.15;95%CI:0.61-2.13,Pvalue 0.08).
Laboratory parameters
Most laboratory parameters are within normal range except for decreased LMR and PLR in both groups,while ESR is slightly elevated.The potassium level is also slightly below the normal reference range,with a median of 4 mmol/L in both groups.Most urinary ketones are negative in both groups(92.5% in the non-rotavirusvs93% in the rotavirus group).There is a significant difference in fecal leukocyte findings between both groups with an OR of 0.33(95%CI:0.17-0.65,Pvalue 0.002)(Tables 1 and 2).
Multivariate logistic regression
Multivariate logistic regression analysis adjusted for variables with a p-value of < 0.25 is shown in Table 3.Multivariate analysis shows that wet season(ORadj= 2.5;95%CI:1.3-4.8,Padj= 0.006),LOS ≥ 3 d(ORadj= 5.1;95%CI:1.4-4.8,Padj= 0.015),presence of abdominal pain(ORadj= 3.0;95%CI:1.3-6.8,Padj= 0.007),severe dehydration(ORadj= 2.9;95%CI:1.1-7.9,Padj= 0.034),abnormal white blood cell counts(ORadj= 2.8;95%CI:1.3-6.0,Padj= 0.006),abnormal random blood glucose(ORadj= 2.3;95%CI:1.2-4.4,Padj= 0.018)and presence of fecal leukocytes(ORadj= 4.1,95%CI:1.7-9.5,Padj= 0.001)are predictors of rotavirus diarrhea.The Hosmer-Lemeshow test shows this model is a good fit with a p-value of 0.361.The AUC for this model is 0.819(95%CI:= 0.746-0.878,Pvalue < 0.001),which shows that this model has good discrimination(Figure 1).

Table 3 Results from multivariate logistic regression analysis for rotavirus diarrhea
DISCUSSION
Comparison with other studies
Rotavirus was shown to be the leading cause of morbidity and mortality in children,especially five years old and below[13].Symptoms tend to be most severe in children between 3-24 mo old.However,in approximately 25% of rotavirus cases,severe disease occurs after two years of age.Serologic evidence of rotavirus infection can be virtually observed in all children aged 4-5[12].Our results showed that our samples have a median age of 1.3 years old.In multivariate analysis,the wet season showed a significant association with rotavirus infection.A previous study showed that in the tropics,rotavirus infection tends to occur all year round compared to the seasonal pattern of infection in countries with temperate climates.However,factors other than temperature,such as rainfall and humidity,play a significant role in rotavirus incidence in the tropics.Due to the waterborne nature of rotavirus transmission,the outbreak pattern might be altered by precipitation levels[14].In low-income areas,stagnant water sources and poor access to uncontaminated water and sanitation were hypothesised to pose a higher risk for rotavirus infection[15].Study showed that monsoon season was significantly correlated with dehydrating rotavirus diarrhea among children aged 0-59 mo in South Asia[16].Previous meta-analyses have also concluded that every 1'C increase in temperature is associated with a 4%-10% decrease in rotavirus infection incidence in the tropics.However,for every one-centimetre increase in mean monthly rainfall and 1% increase in relative humidity(22%),rotavirus incidence decreased by 1% and 3%,respectively.Based on the evidence,it was previously concluded that rotavirus incidence in the tropics was the highest during colder and drier times of the year[17].
Gastroenteritis is generally more severe in the rotavirus group than in the non-rotavirus sample.Length of stay was shown to be prolonged in children age below two years old with rotavirus gastroenteritis.Prolonged LOS,especially in pediatric patients,promote work absenteeism in 70% of parents and could negatively impact the quality of life[18].Prolonged LOS ≥ 3 d is significantly associated with rotavirus gastroenteritis in this study.
Rotavirus has a broad spectrum of symptoms after 1 to 3 d of incubation,varying from subclinical illness to severe dehydration,shock and death.Rotavirus infection has a similar but more severe clinical manifestation than other gastrointestinal infections.Diagnosis of rotavirus gastroenteritis is commonly clinical based on the presence of vomiting and low-grade fever,followed by watery,non-bloody diarrhea.Moderate fever(temperature < 39°C)is found in approximately one-third of infected patients.Fever and vomiting frequently cease within 1 to 3 d.This finding explains our findings that prolonged fever and vomiting are not significantly associated with rotavirus gastroenteritis.Other physical findings such as abdominal cramping,fatigue and signs of dehydration might also occur during the 5 to 7 d disease course.Diagnosis can be further established by the absence of atypical features such as high-grade fever,which is more commonly present in bacterial gastroenteritis,projectile vomiting,bilious vomiting,blood or mucus in stool,persistent diarrhea for more than seven days,focal abdominal pain,absent bowel sound,and history of antibiotic use[4,19,20].Presence of abdominal pain and severe dehydration was associated with rotavirus infection in this study.These findings correlate with findings from the previous study that rotavirus-positive subjects were more likely to present with severe dehydration and tend to require intravenous rehydration therapy than rotavirus-negative subjects[16].However,the role of abdominal pain as a predictor of rotavirus infection is still controversial.Abdominal pain is hypothesised to be limited in rotavirus infection due to low inflammatory response demonstrated by minimal elevation of C-reactive protein or calprotectin levels as clinical markers of inflammation.Rotavirus replication appears to be limited exclusively in the villous epithelium of small intestines,and the diarrhea was considered malabsorptive secondary to enterocyte destruction.Despite non-specific symptomatology,severe abdominal pain and tenesmus tend to indicate large intestines involvement[21,22].Previous studies demonstrated that abdominal pain is particularly frequent in rotavirus-positive subjects or co-infection with rotavirus subjects.However,no significant association has been found in statistical analyses[23].Ambiguous interpretation of abdominal pain by parents of young children during history taking could lead to a bias in pain assessment.This finding might explain the contradictory result regarding abdominal pain in this study.
Rotavirus diarrhea and laboratory values
In this study,rotavirus-positive patients demonstrated abnormal white blood cell counts and abnormal random blood glucose.However,previous studies showed no significant difference in white blood cell count between the rotaviruspositive and rotavirus-negative groups.These studies did not mainly compare rotavirus and the specific etiologic agent of gastroenteritis[24-26].The wide causative range of non-rotavirus gastroenteritis might explain the different findings.Other more significant variables to be compared with rotavirus are indicators of metabolic acidosis secondary to fluid loss.A previous study showed that rotavirus-positive subjects had lower blood pH,higher base deficit,and lower bicarbonate[25].Complete blood count examination appears to have minimal value in predicting rotavirus infection.
Rotavirus diarrhea and respiratory symptoms
Several reports have stated that respiratory symptoms might also occur during the rotavirus infection course.However,the mechanism that explains this finding is still controversial.Coincidental infection with respiratory viruses during rotavirus endemic season might manifest as respiratory symptoms.Previous studies have indicated that rotavirus might infect extra-intestinal organs during viremia,but there has not been sufficient evidence to prove its replication ability outside the intestine.Rotavirus antigens or RNA were detected in the spleen,heart,kidneys,testes,bladder,liver,cells or secretions from the respiratory tract,and endothelial cells[20,27].Our result showed that respiratory symptoms do not predict rotavirus infection in children.Stool analyses in rotavirus-positive subjects are common without blood or white blood cells[20].This result correlates with our findings that faecal leukocytes are a predictor of rotavirus infection.The presence of fecal leucocytes in rotavirus infection may indicate inflammatory processes in the intestines[28].No other hematologic findings were significantly correlated with rotavirus infection in this study.
Limitation
This study has its limitations.Our research is a cross-sectional study to start with.As a result,we could not account for some factors that might affect the severity of rotavirus diarrhea,such as birth weight,source of water,and housecrowding status.Second,the study's focus on just two institutions raises the possibility that this study may not be generalisable to other centres.However,given the nature of the two different hospitals,we were able to include kids from a range of racial and ethnic backgrounds,assuring that both high-and low-income parents were represented in this study.Some variables have insufficient strength for analysis due to missing or unanalysed laboratory data.Third,we could not account for any temporal changes occurring in the four years of the study period.Any seasonality,changes in guidelines and diagnosis of rotavirus diarrhea,as well as immunization update may have altered the results of the study.Lastly,we did not analyse the antigenic properties of the rotavirus due to limited equipment and funding.
CONCLUSION
In this study,wet season,LOS ≥ 3 d,presence of abdominal pain,severe dehydration,abnormal white blood cell counts,abnormal random blood glucose and presence of fecal leukocytes predict rotavirus diarrhea.Since these parameters have good discrimination,these findings should alert clinicians to the presence of rotavirus diarrhea.Clinicians may use these parameters to further alert them to the possibility of rotavirus diarrhea in children and order tests more prudently as well as prescribing appropriate therapy.
ARTICLE HIGHLIGHTS
Research background
Rotavirus gastroenteritis accounted for 19.11% of diarrheal deaths worldwide in 2019 and is still a leading cause of morbidity and mortality,especially in children under five.Surveillance data from 2008-2018 showed that 40.78% of all diarrheal diseases in children in Southeast Asia were attributable to rotavirus infection.
Research motivation
Rotavirus diarrhea is still a leading cause of mortality among Indonesian children.However,since antigen detection is not affordable amongst many families,other cheap clinical proxies for rotavirus diarrhea must be determined.
Research objectives
This study aims to determine clinical and laboratory values that may serve as an indicator to raise clinicians' awareness about rotavirus diarrhea.
Research methods
This study was cross-sectional,with medical records obtained from December 2015 to December 2019 from Siloam General Hospital and Siloam Hospital Lippo Village.Inclusion criteria for this study include all hospitalised pediatric patients(0-18 years old)diagnosed with suspected rotavirus diarrhea,defined as the passing of ≥ 3 watery or loose stools each day.We collected demographic data such as age,gender,and nutritional status.Clinical signs such as temperature upon arrival,vital signs,clinical manifestations(abdominal pain,respiratory symptoms,dehydration status according to World Health Organization),duration and frequency of symptoms(diarrhea,vomiting,fever),length of stay(LOS),treatment given during hospitalisation [intravenous(IV)rehydration and any antibiotics],rotavirus vaccination status,as well as the seasons during which the children contracted diarrhea.
Research results
This study included 267 participants with 187(70%)rotavirus-diarrhea cases.The patients were primarily male in both rotavirus(65.2%)and non-rotavirus(62.5%)groups.The median age is 1.33 years old(0.08-17.67 years old).Multivariate analysis shows that wet season(ORadj= 2.5;95%CI:1.3-4.8,Padj= 0.006),LOS ≥ 3 d(ORadj= 5.1;95%CI:1.4-4.8,Padj= 0.015),presence of abdominal pain(ORadj= 3.0;95%CI:1.3-6.8,Padj= 0.007),severe dehydration(ORadj= 2.9;95%CI:1.1-7.9,Padj=0.034),abnormal white blood cell counts(ORadj= 2.8;95%CI:1.3-6.0,Padj= 0.006),abnormal random blood glucose(ORadj=2.3;95%CI:1.2-4.4,Padj= 0.018)and presence of fecal leukocytes(ORadj= 4.1,95%CI:1.7-9.5,Padj= 0.001)are predictors of rotavirus diarrhea.The area under the curve for this model is 0.819(95%CI:= 0.746-0.878,P value < 0.001),which shows that this model has good discrimination.
Research conclusions
In this study,wet season,LOS ≥ 3 d,presence of abdominal pain,severe dehydration,abnormal white blood cell counts,abnormal random blood glucose and presence of fecal leukocytes predict rotavirus diarrhea.Since these parameters have good discrimination,these findings should alert clinicians to the presence of rotavirus diarrhea.Clinicians may use these parameters to further alert them to the possibility of rotavirus diarrhea in children and order tests more prudently as well as prescribing appropriate therapy.
Research perspectives
More bigger and confirmatory studies are needed to confirm our findings.
FOOTNOTES
Author contributions:Octavius GS and Widjaja M designed the research study;Indrawan M,Chendana J,Handoko TGH,and Octavius GS performed the research;Indrawan M and Chendana J gathered and analyzed the data;Indrawan M,Chendana J,Octavius GS,and Handoko TGH wrote the draft;All authors have read,edited and approved the final manuscript.
Institutional review board statement:This study protocol was approved by the Committee on Ethics at the University of Pelita Harapan,Tangerang,Indonesia,with Code Ethic No.430/FK-UPH/Ext./V/2019.
Informed consent statement:The ethical board exempted informed consent due to the retrospective nature of our study.Identities were removed entirely,and data were analysed anonymously.
Conflict-of-interest statement:All the authors declare that they have no conflict of interest.
Data sharing statement:Data is available upon reasonable request.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BY-NC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Indonesia
ORCID number:Michelle Indrawan 0000-0002-2198-1472;Jason Chendana 0009-0003-4939-7627;Gilbert Sterling Octavius 0000-0002-6439-6265.
S-Editor:Liu JH
L-Editor:A
P-Editor:Zhang XD
 World Journal of Clinical Pediatrics2023年5期
World Journal of Clinical Pediatrics2023年5期
- World Journal of Clinical Pediatrics的其它文章
- Situs inversus totalis in an asymptomatic adolescent-importance of patient education:A case report
- Comments by opponents on the British Medical Association’s guidance on non-therapeutic male circumcision of children seem one-sided and may undermine public health
- Prediabetes in children and adolescents:An updated review
- Pre-autism:What a paediatrician should know about early diagnosis of autism
- Renal calcification in children with renal tubular acidosis:What a paediatrician should know
- Brain metabolic profile assessed by magnetic resonance spectroscopy in children with Down syndrome:Relation to intelligence quotient