
Laparoscopic vs open surgery for gastric cancer: Assessing time,recovery,complications,and markers
2024-03-07 02:57YunYaoLuYunXiaoLiMengHeYaLiWang
Yun-Yao Lu,Yun-Xiao Li,Meng He,Ya-Li Wang
Abstract BACKGROUND Gastric cancer (GC) is one of the most common cancers worldwide.Morbidity and mortality have increased in recent years,making it an urgent issue to address.Laparoscopic radical surgery (LRS) is a crucial method for treating patients with GC;However,its influence on tumor markers is still under investigation.AIM To determine the effects of LRS on patients with GC and their serum tumor markers.METHODS The data of 194 patients treated at Chongqing University Cancer Hospital between January 2018 and January 2019 were retrospectively analyzed.Patients who underwent traditional open surgery and LRS were assigned to the control (n=90) and observation groups (n=104),respectively.Independent sample t-tests and χ2 tests were used to compare the two groups based on clinical efficacy,changes in tumor marker levels after treatment,clinical data,and the incidence of postoperative complications.To investigate the association between tumor marker levels and clinical efficacy in patients with GC,three-year recurrence rates in the two groups were compared.RESULTS Patients in the observation group had a shorter duration of operation,less intraoperative blood loss,an earlier postoperative eating time,and a shorter hospital stay than those in the control group (P < 0.05).No significant difference was observed between the two groups regarding the number of lymph node dissections (P > 0.05).After treatment,the overall response rate in the control group was significantly lower than that in the observation group (P=0.001).Furthermore,after treatment,the levels of carbohydrate antigen 19-9,cancer antigen 72-4,carcinoembryonic antigen,and cancer antigen 125 decreased significantly.The observation group also exhibited a significantly lower incidence rate of postoperative complications compared to the control group (P < 0.001).Additionally,the two groups did not significantly differ in terms of three-year survival and recurrence rates (P > 0.05).CONCLUSION LRS effectively treats early gastric cancer by reducing intraoperative bleeding,length of hospital stays,and postoperative complications.It also significantly lowers tumor marker levels,thus improving the short-term prognosis of the disease.
Key Words: Laparoscopic radical surgery;Gastric cancer;Serum tumor markers;Prognosis;Recurrence;Intraoperative bleeding
lNTRODUCTlON
Gastric cancer (GC),a malignancy affecting the gastrointestinal tract,stands as a leading cause of cancer-related fatalities worldwide[1].According to statistics,> 400000 people in China suffer from GC annually.GC accounts for > 20% of total mortality caused by malignant tumors,with increasing annual incidence and mortality rates[2].The disease often has no obvious clinical symptoms in the early phase and is easily confused with chronic diseases such as gastritis;therefore,most patients are diagnosed in the progressive stage.Early GC usually refers to a tumor with lesions confined to the mucosa or submucosa,with no direct relationship with lesion diameter or lymph node metastasis[3].
Factors such as precancerous lesions,Helicobacter pyloriinfection,poor lifestyle and dietary habits,and regional environmental factors have strong associations with GC development[3].Measures such as improving eating habits,maintaining a good lifestyle,regular stomach examinations,and awareness of hereditary factors can help lower the risk of developing GC[4].Further,factors such as tumor location,pathology,and biological behaviors impact the prognosis of patients with GC.Early radical surgery has the potential to enhance prognosis and prolong survival over 3–5 years[5].
Currently,radical surgery is the primary treatment choice for GC,especially in cases of early-stage GC[5].Commonly adopted surgical methods include open and laparoscopic surgeries.Open surgery can effectively remove tumors at metastatic sites,resulting in a better prognosis;however,it is associated with significant trauma,which is not conducive to postoperative recovery[6,7].Recently,local,and foreign general surgeons have extensively adopted advanced laparoscopic surgical technology[8].With significant advantages in cutting off blood vessels and dissecting lymph nodes,laparoscopic radical surgery (LRS) can reduce surgical trauma and provide a higher anatomical resolution for surgeons[9].Further,LRS may somewhat lower the risk of postoperative complications in patients with GC[10].Accordingly,it is considered an effective and promising treatment method.
Tumor markers refer to substances produced during tumor development and progression,whose levels are used to judge their presence and stage of progression[11].Tumor markers are crucial for tumor-based early screening,diagnosis,treatment effect evaluation,and disease monitoring.However,the effect of LRS on tumor marker levels is still under investigation.
This study aimed to determine the effects of LRS on serum levels of tumor markers in patients with GC,and hence provide a reference for clinical efficacy evaluation.
MATERlALS AND METHODS
General data
Data from 355 patients with GC treated at the Chongqing University Cancer Hospital between January 2018 and January 2019 were retrospectively analyzed.
Inclusion criteria: (1) All patients confirmed gastric cancer by pathological examination;(2) Patients with complete relevant data during hospitalization;(3) Patients who met the indications for surgical treatment;(4) Patients with a Karnofsky function score ≥ 60 points;and (5) Patients who understood the study and agreed to participate in it voluntarily.
Exclusion criteria: (1) Patients with other tumor-related diseases;(2) Patients with immune system diseases;(3) Patients with severe liver or kidney dysfunction;(4) Patients with mental disorders;and (5) Patients unable to communicate normally.
A total of 194 patients who met the inclusion criteria were enrolled.Patients who underwent traditional open surgery and LRS were assigned to the control (n=90) and observation groups (n=104),respectively.
Collection of clinical indexes
The clinical and laboratory examination data of the patients were collected using our hospital’s laboratory information system.Clinical data included sex,age,body mass index (BMI),American Society of Anesthesiologists (ASA) classification score,history of abdominal surgery,and medical history.General information included operation time,intraoperative blood loss,number of lymph node dissections,postoperative complications,postoperative eating time,length of hospital stays,and recurrence rates within 3 years.Laboratory indicators included carbohydrate antigen 19-9 (CA19-9),carbohydrate antigen 72-4 (CA72-4),serum carcinoembryonic antigen (CEA),and carbohydrate antigen 125 (CA125).
Evaluation criteria for efficacy
Markedly effective: After treatment,symptoms such as pain disappeared completely,without complications during the perioperative period,and the tumor was completely removed,with negative cancer cell biopsy lasting for > 1 mo.
Effective: Clinical symptoms were alleviated without complications during the perioperative period,and the tumor shrank by 50%,with negative cancer cell biopsy lasting for ≤ 1 mo.
Outcome measures
Comparison of treatment efficacies and tumor marker level alterations post-treatment between the two groups.Comparative analysis of clinical and general data of the two groups,along with a comparison of the incidence of postoperative complications.Investigation of the association between tumor markers and clinical efficacy by comparing the three-year recurrence rates in the two groups.
Statistical analyses
Based on the retrieved literature on the efficacy of surgery for gastric cancer patients (80% for open surgery and 95% for minimally invasive surgery),we can estimate that approximately 73 patients would be needed in each group while maintaining statistical significance (α=0.05) and sufficient statistical efficacy (80%).This estimate is based on theoretical differences,and in practice a larger sample size may be needed to compensate for the possibility of data loss or follow-up failure.Therefore,the actual sample size may be adjusted according to the specifics of the clinical trial (e.g.,feasibility of patient recruitment,expected lost-to-follow-up rate,etc.).Specifics are collected according to the actual clinical situation.
SPSS 26.0 (IBM,Armonk,NY,Unted States) and GraphPad Prism 9 (GraphPad Software,San Diego,California,Unted States) software were used for data analysis.Counting data were described as rates (percentages),and inter-group comparisons were performed using theχ2test.Measurement data are described as mean ± SD,and inter-group comparisons were conducted using the independent-sample t-test.Receiver operating characteristic curves were drawn to analyze the levels of the tumor markers in predicting clinical efficacy.A significance level ofP< 0.05 was chosen to indicate statistical significance.
RESULTS
Clinical data
Based on the comparison of clinical data,the control and observation groups did not differ significantly in sex,age,BMI,ASA score,history of abdominal surgery,or medical history (P> 0.05,Table 1).
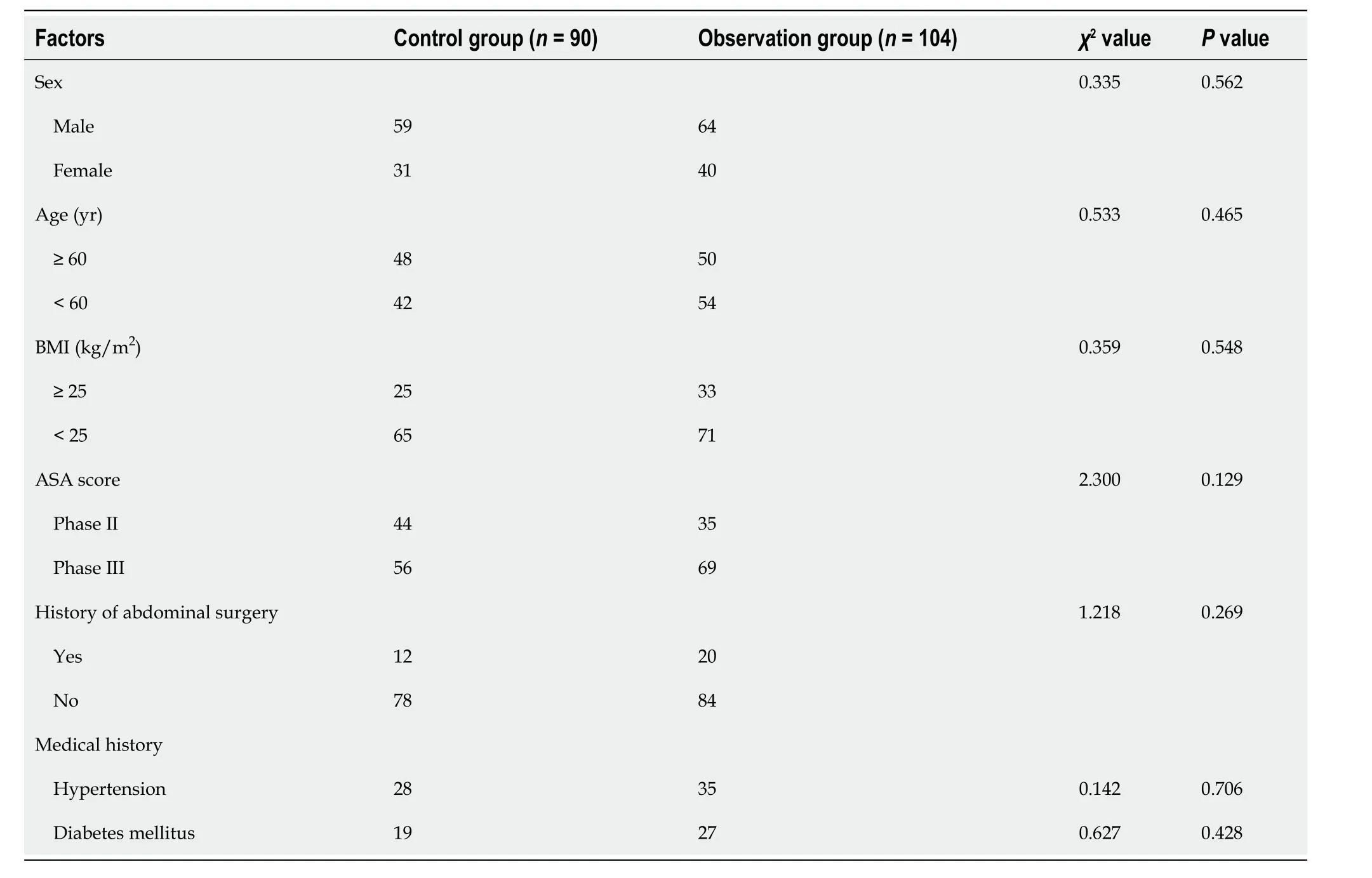
Table 1 Clinical data
General data
Duration of operation,intraoperative blood loss,number of lymph node dissections,postoperative eating time,and length of hospital stay in the two groups were recorded.The patients in the observation group experienced a shorter duration of operation,less intraoperative blood loss,earlier postoperative eating time,and shorter length of hospital stay than those in the control group (P< 0.05,Figure 1).However,the number of lymph node dissections did not significantly differ between the two groups (P> 0.05).
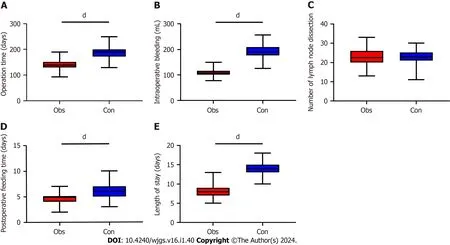
Figure 1 Comparison of general data of patients before and after operation. A-E: The factors compared were Operation time (A);intraoperative blood loss (B);number of lymph node dissections (C);postoperative eating time (D);and length of hospital stay (E).dP < 0.0001.
Clinical efficacy
Based on evaluated clinical efficacy in the two groups,the patients in the control group showed a significantly lower overall response rate than those in the observation group (P=0.001;Table 2).

Table 2 Clinical efficacy evaluation
Changes in tumor marker levels
Tumor marker (CA19-9,CA72-4,CEA,and CA125) levels were compared between the two groups.Before treatment,the two groups had similar levels of CA19-9,CA72-4,CEA,and CA125 (P>0.05),which decreased significantly after treatment (P< 0.001);tumor marker levels in the observation group were lower than those in the control group (P< 0.001,Figure 2).

Figure 2 Changes in the levels of tumor markers in patients before and after treatment.A-D: The markers whose levels before and after treatment were compared include: CA19-9 (A);CA72-4 (B);CEA (C);and CA125 (D).CA19-9: Carbohydrate antigen 19-9;CA72-4: Carbohydrate antigen 72-4;CEA: Serum carcinoembryonic antigen;CA125: Carbohydrate antigen 125.dP < 0.0001.
Statistical analysis of postoperative complications
Statistical analysis of the postoperative complications in the two groups revealed a lower incidence of postoperative complications in the observation group than in the control group (P< 0.001;Table 3).
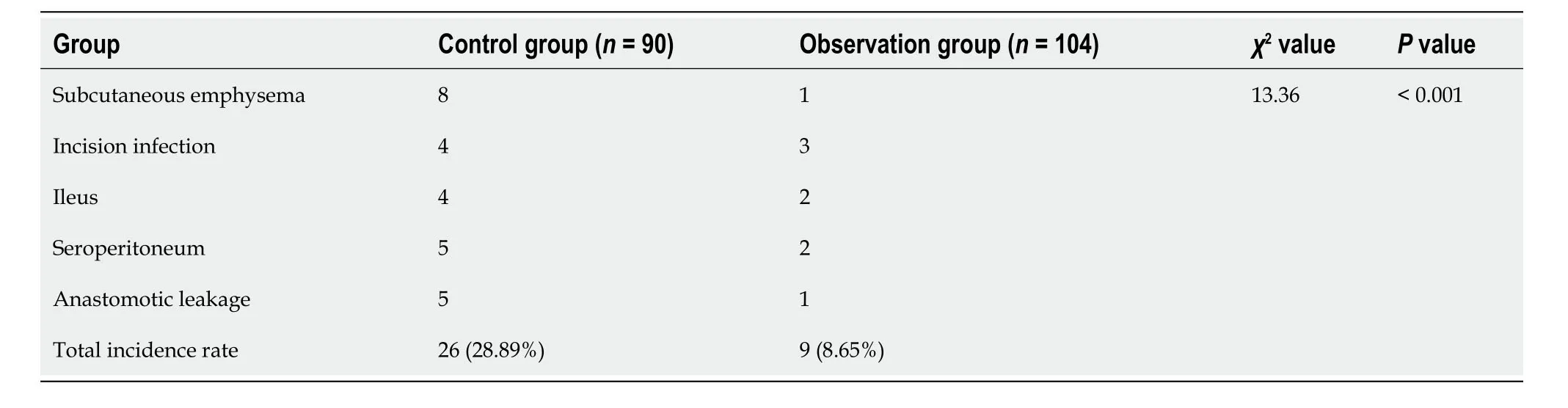
Table 3 Complications
Comparison of recurrence rates in the patients
Three-year follow-up showed that recurrence rates were comparable between the two groups,with the observation group at 20% and the control group at 22%.Thus,no significant difference was found (P> 0.05,Table 4).

Table 4 Comparison of recurrence and survival rates
DlSCUSSlON
For early GC,surgical treatment is mainly performed in clinical practice[12].Open surgery can directly remove the focus lesion;however,it results in higher incidence of complications owing to large trauma,more intraoperative bleeding,long recovery time,poor prognosis,complex tissue structure around the stomach,difficult operation procedure,and long exposure time of the organs[13,14].Therefore,developing a surgical method with less trauma,quick recovery,and minimal impact on immunity is of great practical importance.Laparoscopic surgery is minimally invasive and has become a commonly adopted method for treating GC after several years of development[15].This study is the first to compare the effects of open and laparoscopic surgeries in patients.Here,patients in the observation group had a shorter duration of operation,less intraoperative blood loss,earlier postoperative eating time,and shorter length of hospital stay with a higher overall response rate than those in the control group;however,the two groups did not significantly differ in the number of lymph node dissections.These results imply that LRS shortens the duration of operation,reduces intraoperative blood loss,and accelerates postoperative recovery of gastrointestinal function.According to Kimet al[16],found that,patients who underwent LRS had a shorter recovery duration and a near-ideal surgical effect,consistent with the results of this study.This may be possible because treating GC using LRS guided by an endoscope enables surgeons to observe the anatomical structure of the stomach and its surrounding tissues clearly,allowing for quick and accurate separation of the anatomical level and cleaning of more lymph nodes.In addition,laparoscopic surgery is minimallyinvasive,shortening the operational duration of laparotomy and abdominal closure and reducing abdominal nerve and muscle injury,as well as mechanical traction injury of abdominal organs.Intraoperative blood loss is lower and postoperative pain is milder,promoting postoperative gastrointestinal function recovery.In addition,in this study,the observation group had a lower incidence of postoperative complications than the control group,which was mainly due to lower trauma and stress response after LRS.
Tumor markers are biological substances associated with tumor growth,development,and metastasis.They mainly include proteins,enzymes,genes,antigens,and hormones produced by tumor cells or surrounding tissues,which can be detected in the blood,urine,tissue,and other body fluids[17].Tumor markers have important clinical applications inmany areas,such as early screening,diagnosis,efficacy monitoring,and prognosis evaluation[18].CA19-9 is a glycoprotein tumor marker present in trace amounts or absent in healthy people.In cases of digestive tract infections or tumors,CA19-9 levels increase,which are closely associated with GC progression[19].CA72-4 is a high-molecular-weight glycoprotein antigen sensitive to most malignant gastrointestinal tumors;it is commonly adopted as a marker of these tumors[20].CEA is an acidic protein.After metabolism,tumor cells break away from the surface and enter blood circulation[21,22].CA-125 is not a specific tumor marker but is related to diagnosis,efficacy evaluation,and prognosis of GC.Increased serum levels of CA-125 in some patients with GC are associated with disease progression and metastasis[23].After treatment,changes in CA-125 levels may reflect treatment efficacy and improvement or deterioration of the disease condition.In this study,after treatment,CA19-9,CA72-4,CEA,and CA125 levels in the enrolled patients notably decreased.The reduction was significantly more pronounced in the observation group compared to the control group,indicating that LRS was more effective in treating GC.This may be because laparoscopic surgery can effectively remove focus lesions and lymphoid tissue,thus reducing the secretion of tumor-related markers.
Finally,we performed a statistical analysis of survival and recurrence rates in the two groups.The results revealed no significant differences in three-year survival and recurrence rates between the two groups.In patients with advanced GC,LRS can lower the incidence of postoperative complications and contribute to a favorable long-term prognosis.However,this study has some limitations.First,in this single-center study,the number of samples was greatly reduced after screening,which may have introduced bias in the result analysis.Second,we could not perform long-term follow-up on the patients due to the retrospective nature of the study.Therefore,we hope to perform further experiments with more participants to validate our conclusions.
CONCLUSlON
In summary,LRS is effective in the treatment of early-stage GC,and can reduce intraoperative bleeding,length of stay,and complications,contribute to a good short-term prognosis,and greatly lower tumor marker levels.To further validate these findings,future research with long-term follow-up and a larger sample size should be conducted.
ARTlCLE HlGHLlGHTS
Research background
Gastric cancer (GC) is a common malignancy with increasing incidence owing to lifestyle changes.This study compared the outcomes of open surgery and laparoscopic radical surgery (LRS),two different surgical techniques used to treat early-stage GC.
Research motivation
The need to find an effective and less invasive surgical method with less trauma,quick recovery,and minimal impact on immunity motivated this study.
Research objectives
The primary objectives of this study were to compare the effects of open surgery and LRS on operation time,intraoperative blood loss,postoperative recovery,length of hospital stay,complications,and tumor marker levels in patients with GC.
Research methods
A comparative study was conducted on two groups of patients: one group underwent open surgery and the other,LRS.Surgical time,intraoperative blood loss,postoperative eating time,length of hospital stays,overall response rate,incidence of complications,tumor marker levels (carbohydrate antigen 19-9,cancer antigen 72-4,carcinoembryonic antigen,and cancer antigen 125),and survival and recurrence rates were compared.
Research results
Patients in the LRS group experienced shorter operation times,less intraoperative blood loss,earlier postoperative eating times,and shorter hospital stays,with a higher overall response rate,lower incidence of complications,and significantly decreased tumor marker levels compared with those in the open surgery group.However,no notable differences in three-year survival and recurrence rates were observed between the two groups.
Research conclusions
LRS is an effective treatment for early-stage GC.It offers several advantages over open surgery,including reduced intraoperative bleeding,shorter hospital stays,fewer complications,and lower levels of tumor markers.Even in advanced GC,LRS can reduce postoperative complications and contribute to a favorable long-term prognosis.
Research perspectives
Despite the promising results,the study has limitations,such as a reduced number of samples and a lack of long-term follow-up due to its retrospective nature.Future studies with larger sample sizes and longer follow-up periods are warranted to validate these findings.
FOOTNOTES
Co-first authors:Yun-Yao Lu and Yun-Xiao Li.
Co-corresponding authors:Ya-Li Wang and Meng He.
Author contributions:Lu YY designed and performed the research and wrote the manuscript;Wang YL designed the study and supervised the report;Li YX designed the study and participated in the analysis;He M provided clinical advice and supervised the report;All authors were involved in the critical review of the results and have contributed to,read,and approved the final manuscript.Lu YY and Li YX contributed equally to this work and are the first co-authors.Wang YL and He M contributed equally to this study and are co-corresponding authors.There are two reasons for designating Lu YY and Li YX as co-first authors,and Wang YL and He M as cocorresponding authors.First,the research was performed as a collaborative effort,and the designation of co-first authors and cocorresponding authors accurately reflects the distribution of responsibilities and burdens associated with the time and effort required to complete the study and the resultant paper.This also ensures effective communication and management of post-submission matters,ultimately enhancing the paper's quality and reliability.Second,they contributed efforts of equal substance throughout the research process.The choice of these researchers as co-first authors and co-corresponding authors acknowledges and respects this equal contribution,while recognizing the spirit of teamwork and collaboration of this study.In summary,we believe that designating Lu YY and Li YX as co-first authors,and Wang YL and He M as co-corresponding authors is fitting for our manuscript as it accurately reflects our team's collaborative spirit and equal contributions.
lnstitutional review board statement:The study was reviewed and approved by the Ethics Committee of the Chongqing University Cancer Hospital (Approval No.CZLS2023170-A).
lnformed consent statement:The authors have applied for exemption from obtaining patients’ informed consent.
Conflict-of-interest statement:The authors declare no conflict of interest.
Data sharing statement:The statistical data used in this study can be obtained from the corresponding author upon request.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Yun-Yao Lu 0000-0002-0962-7593;Yun-Xiao Li 0009-0009-0702-392X;Meng He 0009-0002-2711-2566;Ya-Li Wang 0009-0003-2311-9389.
S-Editor:Lin C
L-Editor:A
P-Editor:Xu ZH
 World Journal of Gastrointestinal Surgery2024年1期
World Journal of Gastrointestinal Surgery2024年1期
- World Journal of Gastrointestinal Surgery的其它文章
- Prospects in the application of ultrasensitive chromosomal aneuploidy detection in precancerous lesions of gastric cancer
- Prognostic value of ultrasound in early arterial complications post liver transplant
- Added value of ratio of cross diameters of the appendix in ultrasound diagnosis of acute appendicitis
- Single-incision laparoscopic transabdominal preperitoneal repair in the treatment of adult female patients with inguinal hernia
- Predictive value of machine learning models for lymph node metastasis in gastric cancer: A two-center study
- Micro-power negative pressure wound technique reduces risk of incision infection following loop ileostomy closure