
Paravertebral block's effect on analgesia and inflammation in advanced gastric cancer patients undergoing transarterial chemoembolization and microwave ablation
2024-03-07 03:15YingFenXiongBenZhongWeiYuFengWangXiaoFengLiCongLiu
Ying-Fen Xiong,Ben-Zhong Wei,Yu-Feng Wang,Xiao-Feng Li,Cong Liu
Abstract BACKGROUND Transarterial chemoembolization (TACE) combined with microwave ablation (MWA) is an effective treatment strategy for patients with advanced gastric cancer and liver metastasis.However,it may cause severe postoperative pain and inflammatory responses.The paravertebral block (PVB) is a regional anesthetic technique that provides analgesia to the thoracic and abdominal regions.AIM To evaluate the effect of PVB on postoperative analgesia and inflammatory response in patients undergoing TACE combined with MWA for advanced gastric cancer and liver metastasis.METHODS Sixty patients were randomly divided into PVB and control groups.The PVB group received ultrasound-guided PVB with 0.375% ropivacaine preoperatively,whereas the control group received intravenous analgesia with sufentanil.The primary outcome was the visual analog scale (VAS) score for pain at 6 h,12 h,24 h,and 48 h after the procedure.Secondary outcomes were the dose of sufentanil used,incidence of adverse events,and levels of inflammatory markers (white blood cell count,neutrophil percentage,C-reactive protein,and procalcitonin) before and after the procedure.RESULTS The PVB group had significantly lower VAS scores at 6 h,12 h,24 h,and 48 h after the procedure compared with the control group (P < 0.05).The PVB group also had a significantly lower consumption of sufentanil and a lower incidence of nausea,vomiting,and respiratory depression than did the control group (P < 0.05).Compared with the control group,the PVB group had significantly lower levels of inflammatory markers 24 h and 48 h after the procedure (P < 0.05).CONCLUSION PVB can effectively reduce postoperative pain and inflammatory responses and improve postoperative comfort and recovery in patients with advanced gastric cancer and liver metastasis treated with TACE combined with MWA.
Key Words: Transarterial chemoembolization;Microwave ablation;Paravertebral block;Visual analog scale;Sufentanil;Inflammatory markers
lNTRODUCTlON
Gastric cancer is one of the most common malignancies worldwide and the third leading cause of cancer-related death[1].Liver metastasis is a common complication of advanced gastric cancer that affects the patient prognosis and quality of life[2].Transarterial chemoembolization (TACE) combined with microwave ablation (MWA) is a minimally invasive treatment that can achieve local tumor control and prolong the survival of patients with gastric cancer and unresectable liver metastases[3,4].However,this treatment may induce severe postoperative pain and inflammatory responses,which may affect patient recovery and outcomes[5,6].
The paravertebral block (PVB) is a regional anesthesia technique that provides analgesia to the thoracic and abdominal regions by blocking the spinal nerves in the paravertebral space[7].PVB has been shown to reduce postoperative pain,opioid consumption,and the side effects of various surgical procedures[8-10].However,few studies have reported the effect of PVB on postoperative analgesia and the inflammatory response in patients undergoing TACE combined with MWA for advanced gastric cancer and liver metastasis.
Therefore,we conducted a randomized controlled trial to compare the effects of PVB with those of intravenous analgesia on postoperative pain and inflammatory response in these patients.We hypothesized that PVB would reduce postoperative pain and inflammatory responses and improve postoperative comfort and recovery.
MATERlALS AND METHODS
This study was approved by the Ethics Committee of our hospital.Written informed consent was obtained from all patients before enrollment.The study was conducted following the principles of the Declaration of Helsinki.
Patients
We enrolled patients who met the following criteria: (1) Aged 18–75 years;(2) diagnosed with advanced gastric cancer and unresectable liver metastasis;(3) scheduled for TACE combined with MWA;(4) American Society of Anesthesiologists (ASA) physical status I–III;(5) no contraindications to PVB or intravenous analgesia;(6) no history of allergy to local anesthetics or opioids;(7) no history of coagulation disorders or anticoagulant therapy;(8) no history of chronic pain or opioid use;(9) no history of infection or inflammation in the paravertebral region;and (10) no history of psychiatric disorders or cognitive impairment.
We excluded patients who met any of the following criteria: (1) Conversion to open surgery during the procedure;(2) failure of PVB or intravenous analgesia;(3) occurrence of severe complications during or after the procedure;and (4) withdrawal of consent or loss of follow-up.
Randomization and blinding
We used a computer-generated random number table to randomly assign patients to the PVB or the control group at a 1:1 ratio.The allocation sequence was concealed in sealed opaque envelopes and opened by an independent researcher before the procedure.The patients,anesthesiologists who performed the PVB,radiologists who performed TACE and MWA,and outcome assessors were blinded to the group allocation.The blind method was maintained using a sham PVB procedure for the control group.The control group received an ultrasound-guided needle insertion into the paravertebral space without the injection of a local anesthetic.The patients,anesthesiologists,radiologists,and outcome assessors were blinded to the group allocation and the presence or absence of local anesthetic injections.
Interventions
All patients underwent standard preoperative preparations,including fasting for 8 h and intravenous hydration.Upon arrival at the interventional radiology suite,standard monitoring was performed,including electrocardiography,noninvasive blood pressure measurement,pulse oximetry,and bispectral index.All patients received intravenous midazolam 0.03 mg/kg and dexmedetomidine 1 μg/kg as sedatives before the procedure.
The PVB group underwent ultrasonography-guided PVB with 0.375% ropivacaine before the procedure.The PVB was performed by an experienced anesthesiologist using a linear probe (6-13 MHz) and a 22-gauge,80-mm needle (Stimuplex?A,B.Braun Melsungen AG,Germany).PVB was performed at the T10-L1 levels on both sides of the spine.The paravertebral space was identified using the loss-of-resistance technique and confirmed by ultrasound visualization of the spread of local anesthetic.Twenty milliliters of 0.375% ropivacaine were injected at each level on each side for a total dose of 150 mg.
The patients in the control group received intravenous sufentanil analgesia before and during the procedures.Sufentanil was administered using a patient-controlled analgesia (PCA) pump (Graseby? 3400,Smiths Medical International Ltd.,United Kingdom) with a bolus dose of 5 μg,a lockout interval of 10 min,and a background infusion of 0.1 μg/kg/h.
TACE,combined with MWA,was performed by two experienced radiologists using standard techniques.A 5-Fr catheter was inserted into the femoral artery and advanced into the celiac trunk or the superior mesenteric artery under fluoroscopic guidance.Selective angiography was performed to identify the arteries feeding the liver metastases.A microcatheter was advanced into the feeding arteries,and a mixture of lipiodol,doxorubicin,and mitomycin C was injected until stasis was achieved.After TACE,MWA was performed using a microwave generator (KY-2000;Kangyou Medical,Nanjing,China) and a 14-gauge antenna (KY-2000-14G-15CM-2.45G;Kangyou Medical).The antenna was inserted into the liver metastases under ultrasound guidance,and ablation was performed until a sufficient safety margin was achieved.This procedure was repeated until all liver metastases had been ablated.
Outcomes
The primary outcome was the visual analog scale (VAS) score for pain at 6 h,12 h,24 h,and 48 h after the procedure.The VAS score is a 10-cm horizontal line with anchors at each end representing no pain (score=0) and the worst pain imaginable (score=10).Patients were asked to mark their pain intensity on a line,and the score was measured using a ruler.
The secondary outcomes were: (1) The consumption of sufentanil during and after the procedure;(2) the incidence of adverse events,such as nausea,vomiting,respiratory depression (respiratory rate < 8 breaths/min or oxygen saturation < 90%),hypotension (systolic blood pressure < 90 mmHg or decrease > 20% from baseline),bradycardia (heart rate < 50 beats/min or decrease > 20% from baseline),and puncture site hematoma;and (3) the levels of inflammatory markers,including white blood cell (WBC) count,neutrophil percentage (NEUT%),C-reactive protein (CRP),and procalcitonin (PCT),before and after the procedure.
Sufentanil consumption was recorded using a PCA pump during and 48 h after the procedure.Radiologists activated the PCA pump during the procedure according to the patient’s pain levels.The PCA pump was activated after the procedure.Sufentanil consumption during the procedure was calculated by subtracting the amount of sufentanil used during anesthesia from the total sufentanil consumption during the procedure.Sufentanil consumption during anesthesia was recorded separately for the control group.The PVB group did not receive sufentanil during anesthesia,and adverse events were recorded through direct observation and patient interviews during and after the procedure until discharge.Inflammatory markers were measured using blood samples obtained preoperatively and 24 and 48 h postoperatively.
Statistical analysis
We calculated that a sample size of 26 patients per group would provide 80% power to detect a difference of 2 points in VAS scores between the two groups with a standard deviation of 2.5 points and a significance level of 0.05.The sample size was increased to 30 patients per group to account for a dropout rate of 10%.Data were analyzed using SPSS software (version 22.0;IBM Corp.,Armonk,NY,United States).The normality of the data was tested using the Kolmogorov-Smirnov test.Categorical data are expressed as frequencies and percentages and compared using the chi-square or Fisher’s exact test.Continuous data were expressed as means ± SD and compared using the independent t-test or the Mann-WhitneyUtest.Repeated-measures analysis of variance (ANOVA) or the Friedman test was used to compare the changes in the VAS score and inflammatory markers over time within and between the groups.Statistical significance was set atP< 0.05.
RESULTS
Sixty patients were enrolled and randomly assigned into one of two groups.Two patients in the control group were excluded due to conversion to open surgery or failure of intravenous analgesia.The final analysis included 28 and 30 patients in the PVB and control groups,respectively.The baseline patient characteristics are shown in Table 1.The groups did not differ significantly in age,sex,body mass index,ASA of anesthesiologist’s physical status,tumor size,number of tumors,or procedure duration.
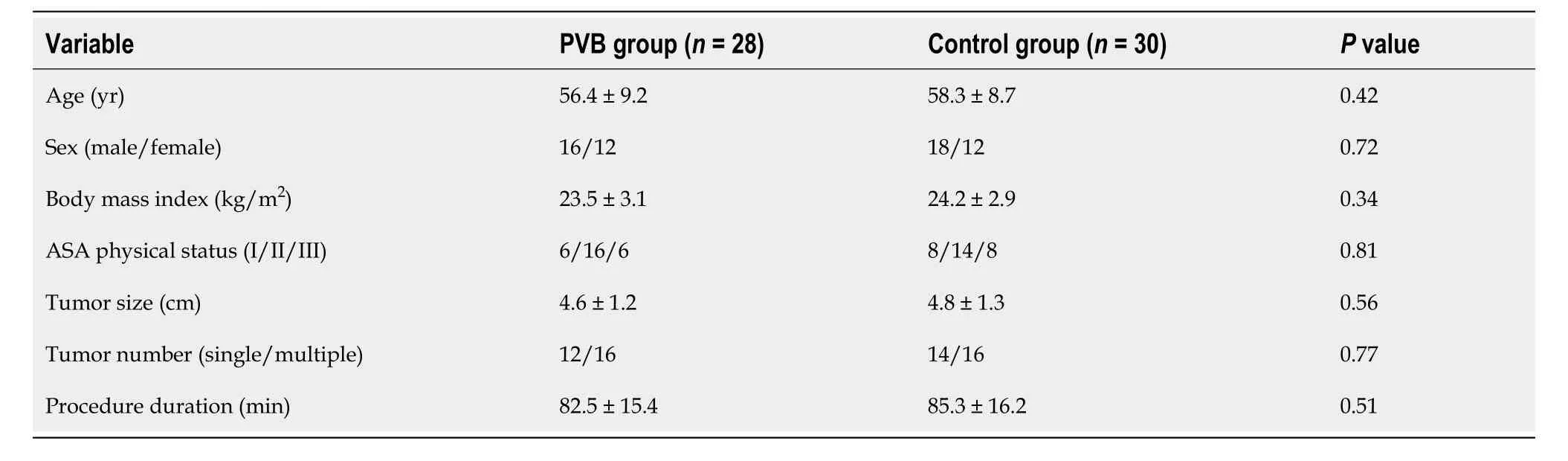
Table 1 Patients’ baseline characteristics
VAS scores for pain at different time points after the procedure are shown in Table 2.The PVB group had significantly lower VAS scores than that in the control group at all time points (P< 0.05).A repeated-measures ANOVA revealed a significant interaction effect between the groups and time (P< 0.001),indicating that the difference in the VAS scores between the two groups changed over time.

Table 2 Visual analog scale score for pain at different time points after the procedure
Sufentanil consumption during and after the procedure is shown in Table 3.The PVB group had a significantly lower consumption of sufentanil than that in the control group during and after the procedure (P< 0.05).

Table 3 Consumption of sufentanil during and after the procedure
The incidence of adverse events during and after the procedure is shown in Table 4.The PVB group had a significantly lower incidence of nausea,vomiting,and respiratory depression than that in the control group (P< 0.05).The groups did not differ significantly regarding the incidence of hypotension,bradycardia,or puncture site hematoma between the two groups (P> 0.05).
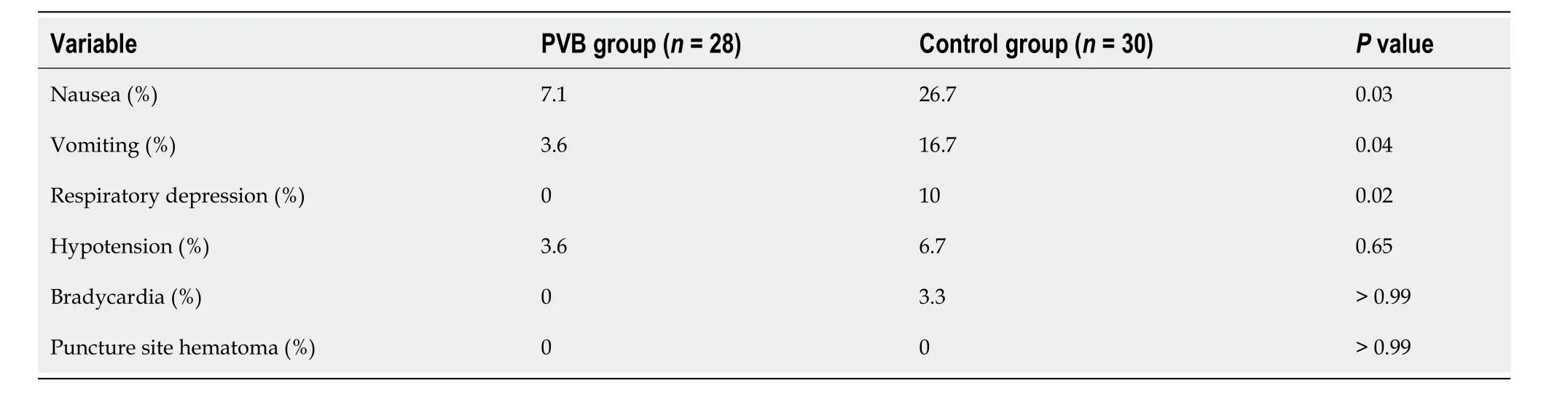
Table 4 lncidence of adverse events during and after the procedure
The levels of inflammatory markers before and after the procedure are shown in Table 5.The PVB group had significantly lower WBC count,NEUT%,CRP,and PCT levels than those in the control group at 24 and 48 h after the procedure (P< 0.05).Repeated measures ANOVA revealed a significant interaction effect between group and time for all inflammatory markers (P< 0.001),indicating that the difference in the inflammatory response between the two groups changed over time.

Table 5 Levels of inflammatory markers before and after the procedure
DlSCUSSlON
This study revealed that PVB can effectively reduce postoperative pain and inflammatory responses in patients with advanced gastric cancer and liver metastasis treated with TACE combined with MWA and improve postoperative comfort and recovery.
Postoperative pain is a common and distressing symptom in patients undergoing TACE combined with MWA and may affect their quality of life and recovery.Postoperative pain may trigger or exacerbate inflammatory responses,which may increase the risk of infection,organ dysfunction,and poor outcomes.Therefore,adequate postoperative analgesia is essential for these patients.
PVB is a regional anesthetic technique that provides analgesia to the thoracic and abdominal regions by blocking the spinal nerves in the paravertebral space.PVB has several advantages over other analgesic methods,such as intravenous,epidural,and intrathecal analgesia[11].First,PVB provides effective and long-lasting analgesia without affecting the motor or sensory functions of the lower limbs[12].Second,PVB can reduce the consumption of opioids and associated side effects such as nausea,vomiting,respiratory depression,pruritus,and constipation[13].Third,PVB can attenuate stress and inflammatory responses induced by surgery or trauma,which may improve immune function and patient outcomes[14].
In this study,PVB significantly reduced the VAS score for pain at all time points after the procedure compared to that in intravenous analgesia,indicating that PVB provides superior postoperative analgesia for these patients[15].This is consistent with the findings of previous studies that reported that PVB can reduce postoperative pain in various surgical procedures involving the thoracic or abdominal regions[16].We observed that PVB significantly reduced the consumption of sufentanil during and after the procedure compared with that in intravenous analgesia,indicating that PVB reduced the need for opioids and their potential side effects[17].This is consistent with the results of previous studies,indicating that PVB can reduce opioid consumption and side effects during various surgical procedures[18,19].
In addition to postoperative analgesia,we evaluated the effect of PVB on the postoperative inflammatory responses in these patients.We measured the levels of inflammatory markers,including WBC count,NEUT%,CRP,and PCT,before and after the procedure.We identified that PVB significantly reduced the levels of inflammatory markers 24 and 48 h after the procedure compared to that in intravenous analgesia,indicating that PVB attenuated the postoperative inflammatory response in these patients.This is in accordance with previous studies showing that PVB reduces the levels of inflammatory markers during various surgical procedures[20-23].The mechanism by which PVB reduces the postoperative inflammatory response may be related to its effect on blocking sympathetic nerve activity and modulating the neuroendocrine-immune axis[24].
Reducing the postoperative inflammatory response caused by PVB may have clinical implications for these patients[25].First,it may reduce the risk of infection,a common complication of TACE combined with MWA[26,27].Second,it may improve organ function and outcomes in these patients because the postoperative inflammatory response is associated with organ dysfunction and mortality[28].Third,it may enhance the antitumor effect in these patients because postoperative inflammatory responses are linked to tumor progression and recurrence[29].
This study had certain limitations that should be acknowledged.First,this was a single-center study with a relatively small sample size,which may limit its generalizability and statistical power.Second,the patients were followed up for only 48 h after the procedure,which might not have reflected the long-term effects of PVB on postoperative recovery and outcomes.Third,we did not measure other outcomes that may have been affected by PVB,such as patient satisfaction,quality of life,length of hospital stay,and survival.
CONCLUSlON
PVB can effectively reduce postoperative pain and inflammatory responses in patients with advanced gastric cancer and liver metastasis treated with TACE combined with MWA and improve postoperative comfort and recovery.We suggest that PVB should be considered as an alternative or adjunctive analgesic method for these patients.Further studies with larger sample sizes and longer follow-up periods are required to validate our findings.
ARTlCLE HlGHLlGHTS
Research background
Transarterial chemoembolization (TACE) combined with microwave ablation (MWA) has emerged as an effective treatment strategy for patients with advanced gastric cancer and liver metastasis.However,this approach often leads to severe postoperative pain and inflammatory responses,impacting patient comfort and recovery.The paravertebral block (PVB) is a regional anesthetic technique known for providing analgesia in the thoracic and abdominal regions.This study aims to evaluate the potential benefits of PVB in terms of postoperative analgesia and inflammatory response in patients undergoing TACE combined with MWA for advanced gastric cancer and liver metastasis.By comparing the outcomes between the PVB group and the control group receiving intravenous analgesia,this research investigates the effectiveness of PVB in reducing pain scores,minimizing sufentanil consumption,decreasing adverse events,and lowering inflammatory marker levels.The findings of this study will shed light on the role of PVB in managing pain and inflammation and improving the postoperative experience and recovery of patients with advanced gastric cancer and liver metastasis treated with TACE combined with MWA.
Research motivation
The treatment of advanced gastric cancer and liver metastasis using TACE combined with MWA has shown promising results.However,the occurrence of severe postoperative pain and inflammatory responses poses significant challenges in patient management.The PVB technique offers a potential solution by providing effective analgesia to the thoracic and abdominal regions.This study aims to investigate the impact of PVB on postoperative pain and inflammation in patients undergoing TACE combined with MWA for advanced gastric cancer and liver metastasis.
Research objectives
The main objective of this study was to evaluate the effect of PVB on postoperative analgesia and inflammatory response in patients undergoing TACE combined with MWA for advanced gastric cancer and liver metastasis.The specific objectives were to compare the visual analog scale (VAS) scores for pain,the dose of sufentanil used,the incidence of adverse events,and the levels of inflammatory markers between the PVB group and the control group.The significance of realizing these objectives is to contribute to improving postoperative comfort and recovery in patients with advanced gastric cancer and liver metastasis treated with TACE combined with MWA,as well as informing future research in this field.
Research methods
This study used a randomized controlled trial design.Sixty patients undergoing TACE combined with MWA for advanced gastric cancer and liver metastasis were randomly divided into two groups: the PVB group and the control group.The PVB group received ultrasound-guided PVB with 0.375% ropivacaine preoperatively,while the control group received intravenous analgesia with sufentanil.The primary outcome measured was the VAS score for pain at specific time points after the procedure.Secondary outcomes included the dose of sufentanil used,incidence of adverse events,and levels of inflammatory markers before and after the procedure.Statistical analyses were performed to compare the outcomes between the two groups.
Research results
The findings of this study demonstrated that patients in the PVB group had significantly lower VAS scores for pain at 6 h,12 h,24 h,and 48 h after the procedure compared to the control group.Additionally,the PVB group showed reduced consumption of sufentanil and a lower incidence of adverse events such as nausea,vomiting,and respiratory depression.Moreover,the PVB group exhibited significantly lower levels of inflammatory markers 24 h and 48 h after the procedure.These results contribute to the understanding of how PVB can effectively alleviate postoperative pain,reduce inflammatory responses,and enhance the comfort and recovery of patients with advanced gastric cancer and liver metastasis treated with TACE combined with MWA.Further research is needed to address any remaining challenges in optimizing the application of PVB in this context.
Research conclusions
That the use of PVB in patients undergoing TACE combined with MWA for advanced gastric cancer and liver metastasis results in effective reduction of postoperative pain and inflammatory responses.Moreover,PVB improves postoperative comfort and enhances recovery.These results support the implementation of PVB as a valuable technique in managing pain and inflammation in this patient population.Further investigations should focus on optimizing the utilization of PVB and exploring its long-term effects on patient outcomes.
Research perspectives
TACE combined with MWA offers promising research prospects for the treatment of advanced cancer and liver metastasis.Further studies can focus on optimizing the technique and dosage of PVB,exploring its long-term impact on patient prognosis,and investigating the potential synergistic benefits when PVB is combined with other analgesic strategies.Additionally,research can investigate the effects of PVB on other aspects such as quality of life,length of hospital stay,and healthcare costs to further evaluate its overall clinical benefits.
FOOTNOTES
Co-first authors:Ying-Fen Xiong and Ben-Zhong Wei.
Author contributions:Xiong YF and Wei BZ proposed the concept of this study;Liu C validated this study;Xiong YF and Wei BZ jointly wrote the first draft;Wang YF contributed to data collection;Li XF contributed to formal analysis;Xiong YF and Wei BZ participated in the survey;Liu C and Li XF contributed to the methods;Wang YF contributed to the visualization of this study.All authors collectively guided the research,reviewed,and edited the manuscript.Xiong YF and Wei BZ have made equal contributions to this work as co-first authors.It has been decided to designate Xiong YF and Wei BZ as co-first authors for three main reasons.Firstly,this study was conducted as a collaborative effort,warranting the designation of co-first authors.The authors accurately reflect the distribution of responsibilities and burdens associated with the time and effort required to complete the research and final manuscript.Designating two co-first authors will ensure effective communication and management of post-submission matters,thereby enhancing the quality and reliability of the paper.Secondly,the co-first authors from the research team possess diverse expertise and skills from different fields,and their designation best reflects this diversity.It also facilitates the most comprehensive and in-depth exploration of the research topic,ultimately enriching readers' understanding by providing various expert perspectives.Thirdly,Xiong YF and Wei BZ have made substantial and equal contributions throughout the research process.Selecting these researchers as co-first authors acknowledges and respects their equal contributions,showcasing the collaborative and teamwork spirit within this study.We believe that designating Xiong YF and Wei BZ as co-first authors is fitting for our manuscript as it accurately reflects the collaborative spirit,equal contributions,and diversity within our team.
lnstitutional review board statement:This study has been reviewed and approved by the Medical Ethics Committee of the First Affiliated Hospital of Nanchang University.
Clinical trial registration statement:This study is registered in https://www.researchregistry.com.The registration identification number is Researchregistry9712.
lnformed consent statement:All study participants,or their legal guardian,provided informed written consent prior to study enrollment.
Conflict-of-interest statement:All authors declare that there is no disclosure of interest relationship.
Data sharing statement:No additional data are available.
CONSORT 2010 statement:The authors have read the CONSORT 2010 statement,and the manuscript was prepared and revised according to the CONSORT 2010 statement.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Ying-Fen Xiong 0009-0007-4996-9807;Ben-Zhong Wei 0009-0002-8751-724X;Cong Liu 0009-0005-1956-1099.
S-Editor:Lin C
L-Editor:A
P-Editor:Che YX
 World Journal of Gastrointestinal Surgery2024年1期
World Journal of Gastrointestinal Surgery2024年1期
- World Journal of Gastrointestinal Surgery的其它文章
- Prospects in the application of ultrasensitive chromosomal aneuploidy detection in precancerous lesions of gastric cancer
- Prognostic value of ultrasound in early arterial complications post liver transplant
- Added value of ratio of cross diameters of the appendix in ultrasound diagnosis of acute appendicitis
- Single-incision laparoscopic transabdominal preperitoneal repair in the treatment of adult female patients with inguinal hernia
- Predictive value of machine learning models for lymph node metastasis in gastric cancer: A two-center study
- Micro-power negative pressure wound technique reduces risk of incision infection following loop ileostomy closure