
Prospective observational study on the prognosis of ureteral lesions caused by impacted stones via dual-energy spectral computed tomography
2024-01-11 11:02JunjieWngXimingWngHozhouZhongWenguiXieQilinXi
Asian Journal of Urology 2023年4期
Junjie Wng , Ximing Wng , Hozhou Zhong , Wengui Xie ,Qilin Xi ,*
a Department of Urology, The Sixth People’s Hospital of Chengdu, Chengdu, China
b Department of Radiology, The First Affiliated Hospital of Soochow University, Suzhou, China
c Department of Urology, The First Affiliated Hospital of Soochow University, Suzhou, China
KEYWORDS Ureteral lesions;Impacted ureteral stone;Dual-energy spectral computed tomography;Ureteral stricture;Ureteroscopic lithotripsy
Abstract Objective: Ureteral lesions caused by impacted ureteral stones are likely to result in postoperative ureteral stricture.On this basis,the study aimed to investigate if dual-energy spectral computed tomography can predict ureteral hardening caused by impacted stones and to explore the relationship between different types of ureteral lesions and the risk of ureteral stricture.Methods: This prospective study collected data of 93 patients with impacted stones from hospital automation system during January 2018 to October 2019.They underwent an abdominal scan on a dual-energy spectral computed tomography.During surgery, the operator used ureteroscopy to identify ureteral lesions, which were classified into four categories: edema,polyps, pallor, and hardening.Seven months later, 90 patients were reviewed for the degree of hydronephrosis.Results: Endoscopic observations revealed 38(41%)cases of ureteral edema,20(22%)cases of polyps,13(14%)cases of pallor,and 22(24%)cases of hardening.There were significant differences in hydronephrosis,the period of impaction,the calcium concentration of the ureter,and the slope of the spectral Hounsfield unit curve between the four groups.After that, we evaluated the factors associated with ureteral hardening and found that the calcium concentration of the ureter and hydronephrosis remained independent predictors of ureteral hardening.Receiver operating characteristic curve analysis showed that 5.3 mg/cm3 calcium concentration of the ureter is an optimal cut-off value to predict ureteral hardening.The result of follow-up showed that 80 patients had complete remission of hydronephrosis,with a complete remission rate of 61.9%(13/21)in the hardening group and 97.1%(67/69)in the non-hardening group (p<0.001).Conclusion: Calcium concentration of the ureter is an independent predictor of ureteral hardening.Patients with ureteral hardening have more severe hydronephrosis after ureteroscopic lithotripsy.When the calcium concentration of the ureter is less than 5.3 mg/cm3,ureteral lesions should be actively treated.
1.Introduction
Kidney stones are a global epidemic with an incidence of 7%-13% in North America, 5%-9% in Europe, and 1%-5% in Asia [1].A recent review showed that the prevalences of kidney stones in three groups were 5.95%,8.86%,and 10.63%in 1991-2000, 2001-2010 and 2011-2017, respectively,suggesting prevalence is an increasing trend [2].With the increasing prevalence of kidney stones, incarcerated impacted stones are also increasing, which causes inflammation in the ureteral mucosa and results in edema and fibrosis,etc.Recent studies have shown that impacted stones are the most common cause of postoperative complications or ureteral strictures [3-5].Mugiya et al.[6] reported that histological examination of ureteral lesions showed chronic inflammation,interstitial fibrosis,and urothelial hyperplasia.
According to existing reports,the possible risk factors for ureteral stricture after ureteroscopic lithotripsy (URSL) are mainly divided into two categories:stone-related factors and surgical-related factors.The former includes stone impaction, stone size, and stone fragments lodged in the ureter mucosa [5,7,8].Surgical-related factors include ureteral perforation, larger ureteroscope diameter (8.5/10 Fr),and high-power holmium settings [4,9,10].We found that ureteral strictures developed postoperatively in some patients despite avoiding surgical-related factors.Therefore,it is necessary to determine which type of ureteral lesion is more likely to become ureteral stricture.We found that ureteral lesions could be classified into four types during surgery, edema, polyps, pallor, and hardening.The appearance of ureteral polyps was villous or showed multiple stripy protrusions.The ureteral mucosa was pale and usually free of polyps in the pallor group.In the hardening group, the ureteral cavity was narrowed, and the tube wall was stiff and appeared to have interstitial fibrosis.However, at present,ureteral lesions cannot be detectedby computedtomography(CT)or magnetic resonance imaging.
Recent rapid technological advances have contributed to the widespread clinical application of dual-energy spectral computed tomography (DECT), which created two views per location at two different energies [11].An additional attenuation measurement is obtained with a second X-ray spectrum(i.e.,a second energy),allowing the differentiation of multiple materials [12].Materials with low and high attenuation, such as water and calcium, are often used as the basis pair for medical diagnostic imaging[11].Currently, many studies have used DECT to analyze tissue components.
The study aimed to investigate if DECT can predict ureteral hardening caused by impacted stones and to explore the relationship between different types of ureteral lesions and the risk of ureteral stricture.
2.Patients and methods
2.1.Study design and patient population
This study was conducted in compliance with the principles of the 1975 Declaration of Helsinki and approved by the Ethics Committees of the First Affiliated Hospital of Soochow University (First Affiliated Hospital of Soochow University 2017 ethical approval No.032).Written informed consents were obtained from all patients or their legal representatives before their participation in the study.
Among the 269 patients admitted for surgical treatment from January 2018 to October 2019, 93 adult patients included in this study had impacted ureteral stones according to the inclusion criteria.They are 67 males and 26 females.Patients ranged in age from 25 years to 76 years,with a mean age of 53 years.
Eligible patients must satisfy one of the following conditions: (a) difficulty in passing a cook guidewire over a stone on the first attempt; (b) moderate to severe hydronephrosis (the anteroposterior diameter of the renal pelvis>10 mm);or(c)stone staying in the same position for more than 2 months (they were medicated for pain without further treatment) [13].Patients with kidney stones were excluded (Fig.1).
2.2.DECT procedure
All patients underwent abdominal DECT scans in spectral mode on DECT (GE Revolution, USA) preoperatively.The scanning parameters were as follows: the fast-kilovoltpeak switching (80 kVp and 140 kVp), the tube current of each scan being 320 mA, gantry rotation speed of 0.5 r/s,field of view display of 250 mm, reconstruction layer thickness of 1.25 mm, and pitch of 0.984 mm.The polychromatic images and a set of monochromatic images were obtained, and spectrum parameters were analyzed on the AW4.6 workstation (GE Revolution, USA).The selection of window width and level were width 250 of center 40.All DECT images were evaluated by an experienced radiologist (Wang X) in a blinded manner for impaction and outcomes.

Figure 1 Participant flow.DECT, dual-energy spectral computed tomography.
Ureteral wall thickness (UWT) and spectral parameters were recorded and measured in the region of interest,first slice distal to the stone [14].Because ureteral lesions usually appear below the stones, Deguchi et al.[15] suggested that a high CT attenuation value of the ureter just below the stone may reflect tissue edema and inflammation, which might be the reason why the calculated Hounsfield unit(HU)above-below ratio is high in cases with impacted ureteral stone.The calcium concentration of the ureter was measured in calcium-based material images.The water concentration of the ureter was measured in water-based material images.The slope of the spectral HU curve and effective atomic number (effective-Z) were also measured and calculated.HU curve indicates the attenuation of the ureter at different levels of energy.The stone size (transverse stone length), stone diameter (longest stone length), location of stones, hydronephrosis, and ureteral thickness were measured in the Picture Archiving and Communication System.Stone size was defined as largest diameter in the transverse section CT images.UWT was defined as the ureteral diameter in the transverse section CT images.Hydronephrosis was defined as the anteroposterior diameter of the renal pelvis.The period of impaction was defined as from the episode of first ureteral stone to hospitalization.
2.3.Retrograde rigid ureteroscopy technique
In our study, retrograde rigid ureteroscopy (8.0/9.8 Fr or 6.0/7.5 Fr, Storz, Germany) and holmium laser lithotripsy system (Da Hua DHL-1-D, Wuxi, Jiangsu, China) with a power of 10-20 W and a rate of 8-10 Hz were used to disintegrate the stones.All operations were performed by an expert urologist.The ureteral stent(6 Fr)was remained for 4 weeks.Patients were reviewed by B-ultrasound to evaluate hydronephrosis 7 months after the operation.
A urologist identified ureteral lesions by ureteroscopy,which are classified into four types: edema, polyps, pallor,and hardening (Fig.2).The appearance of ureteral polyps was villous or showed multiple stripy protrusions.The ureteral mucosa was pale and usually free of polyps in the pallor group.In the hardening group, the ureteral cavity was narrowed,and the tube wall was stiff and appeared to have interstitial fibrosis.If there were two kinds of ureteral lesions,the more severe lesion was used as the lesion type.
2.4.Statistical analysis
Data analysis was performed by IBM SPSS Statistics for Windows, Version 24.0 (IBM, New York, NY, USA).Clinical variables were compared by analysis of variance, the Wilcoxon rank sum test, and the Chi-square test.Factors potentially predictive of hydronephrosis, such as the duration of symptoms,calcium concentration,and the rate of the curve, were determined by multiple logistic regression analysis.The ideal cut-off value predicting the ureteral lesion and its predictive accuracy were determined by the receiver operating characteristic curve analysis.The p-value of less than 0.05 was considered statistically significant.
3.Results
There were 93 eligible out of 269 patients for the present analysis.The male to female ratio was 1.9:1.The endoscopic observations of 38 (41%) patients were ureteral edema; 20 (22%) patients were ureteral polyps; 13 (14%)patients were ureteral pallor; and 22 (24%) patients were ureteral hardening.There was no case of ureteral perforation during the operation.
Table 1 lists the baseline characteristics of the four groups, which were not significantly different with respect to age,sex, stone size,site of impaction, UWT, effective-Z or water concentration.Meanwhile, there were significant differences in hydronephrosis,the period of impaction,the calcium concentration of the ureter, and the slope of the spectral HU curve.
Among the parameters with significant differences, we used the LSD-t test for pairwise comparison and found that hydronephrosis (hardening vs.edema, p<0.001; pallor vs.edema, p=0.018), calcium concentration of the ureter(hardening vs.edema, p<0.001; hardening vs.polyps,p<0.001), rate of curve (hardening vs.edema, p=0.017;hardening vs.polyps, p=0.038), duration of impaction(pallor vs.edema, p=0.037) remained significantly different (Table 2).

Table 1 Baseline characteristics of hardening, pallor, polyps, and edema groups.
The above differences between groups mainly existed between the hardening group and the non-hardening group.Therefore, we evaluated the factors associated with ureteral hardening using multiple logistic regression analysis(Table 3).In this study,Tol of all independent variables are more than 0.1, and there is no collinearity, since variance inflation factor is less than 3.We found that the calcium concentration of the ureter (odds ratio, 0.595; p=0.001)and hydronephrosis (odds ratio, 1.063; p=0.014) remained independent predictors of ureteral hardening.Because the calcium concentration was closely related to ureteral hardening, we focused on this factor.
The receiver operating characteristic curve analysis showed that 5.3 mg/cm3calcium concentration of the ureter is an optimal cut-off value to predict ureteral hardening, with an area under the curve of 0.84 (95% confidence interval,0.72-0.96).This cut-off(5.3 mg/cm3)has a sensitivity of 81.8%and a specificity of 87.3%in predicting ureteral hardening (Fig.3, Table 4).
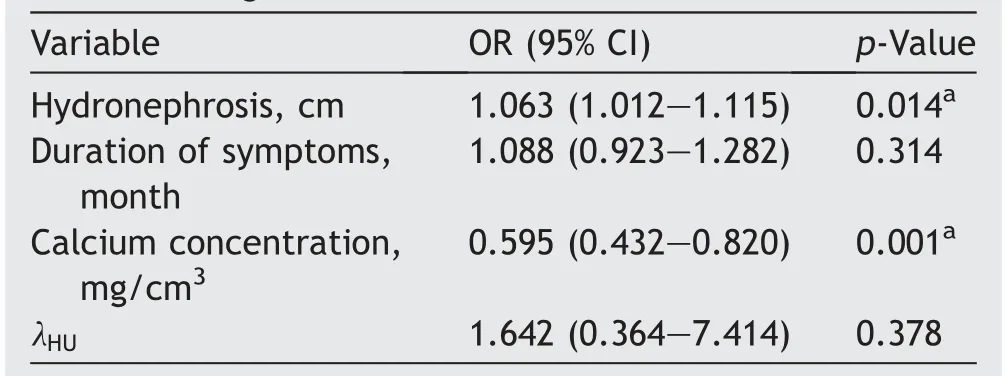
Table 3 Multivariate logistic regression analysis ofpreoperative factors associated with the hardening and non-hardening.
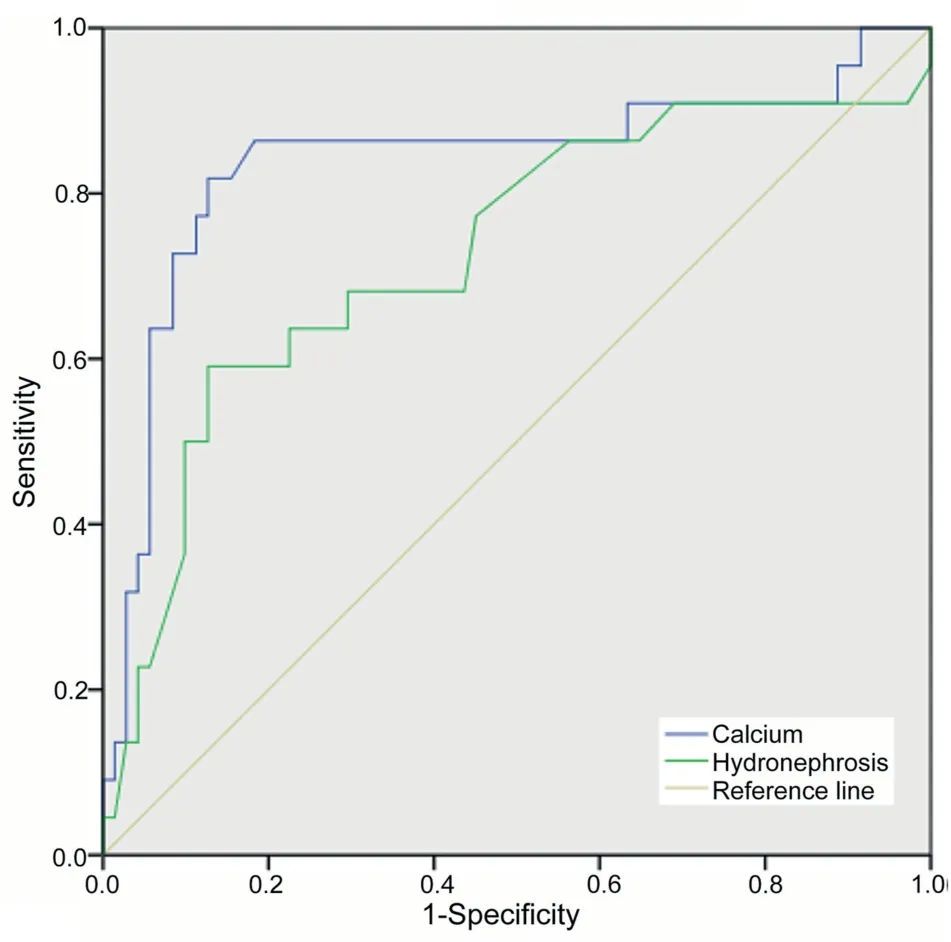
Figure 3 Effect of dual-energy spectral computed tomography calcium concentration of the ureteral wall and hydronephrosis on preoperative prediction of ureteral hardening.
Ninety patients were followed-up by ultrasonography 7 months after surgery;of the three patients who were lost to follow-up, two were in the polyps group and one was in the hardening group.No residual ureteral stones were found in any of the followed-up cases.
Among the 90 patients, 80 patients had complete remission of hydronephrosis, with a complete remission rate of 61.9% (13/21) in the hardening group and 97.1%(67/69)in the non-hardening group(p<0.001).There were eight cases of hydronephrosis with slight remission,including seven cases of hardening and one case of polyps.In addition, the condition of only two patients of hydronephrosis became worsened.One of the two is in the hardening group.This patient had 14 mm of hydronephrosis before the surgery that increased to 42 mm after follow-up.Another patient is in the pallor group.This patient had 22 mm of hydronephrosis before the surgery that increased to 36 mm after follow-up.

Table 4 Distributionofcalciumconcentrationofdual-energy spectral computed tomography in four groups.
4.Discussion
Over the past two decades, the surgical treatment of ureteral stones has changed greatly, and URSL has replaced extracorporeal shock wave lithotripsy as the most common way of treatment [16].URSL has further improved the primary stone clearance rate.However, in recent years, ureteral stricture after URSL is very common, which is a prominent problem worthy of attention.With the development of URSL technology, more advanced equipment has emerged, such as slimmer electronic ureteroscopy,high-frequency holmium laser with adjustable pulse width,and stone basket.At the same time, surgeons should avoid ureteral perforation, choose low energy laser lithotripsy,and maintain good cold-water perfusion to avoid boiling the ureter.However, these changes still cannot completely avoid the occurrence of ureteral stricture after URSL.In addition to surgical factors,a large number of literature has indicated that ureteral lesions caused by impacted stones may be a potential risk factor for postoperative ureteral stricture [4,8,13,17].In the prospective study of Darwish et al.[4], 263 patients after URSL were followed up for an average of 12 months.Finally, urography confirmed four patients with ureteral stricture, including three patients with impacted stones.A retrospective study by Machida et al.[11] showed that 13.3% of patients with impacted stones experienced ureteral stricture after URSL, while only 5% of patients with non-impacted stones experienced stricture (p<0.05).Elashry et al.[18] retrospectively analyzed 3215 patients undergoing URSL, and 12 patients with postoperative ureteral stricture all had incarcerated stones before surgery.
Ureteral stricture is a serious complication that can lead to a series of invasive examinations,secondary surgery,and even damage to kidney function.Therefore, preoperative diagnosis of ureteral hardening that may cause stricture can guide clinicians in making more effective surgical and follow-up plans, thus reducing the harm to patients.For ureteral hardening,the ureteral cavity is narrowed,and the tube wall is stiff.Among the four parameters of DECT,calcium concentration of the ureter is an independent factor to predict ureteral hardening.The lower calcium concentration was consistent with the endoscopic observations of ureteral hardening.In addition, the follow-up results showed that the complete remission rate of hydronephrosis in the hardening group (61.9%) was significantly lower than that in the non-hardening group(97.1%),and the two cases of hydronephrosis aggravation were in the hardening group and pallor group, respectively.This indicates that ureteral hardening is more likely to convert to postoperative ureteral stricture.When the calcium concentration was less than 5.3 mg/cm3, the ureter was considered as hardening, and ureteral stricture was more likely to occur after surgery.Therefore, on the one hand,these patients should be closely followed up after URSL.Once hydronephrosis is found to have aggravation or no relief, further examination and treatment can be conducted immediately [19].On the other hand, combined removal of stones with resection of ureter hardening may achieve satisfactory results [20].Other methods include endoscopic balloon dilation or incision in URSL.
Recently, many studies have found that the attenuation of the ureter and ureteral thickness is the precise preoperative predictor of impacted stones in patients with ureteral stones [5,21,22].The currently existing situation is that ureteral stricture does not occur in all impacted stones.Therefore, we need to find out which kind of impacted stones could cause ureteral stricture.DECT is an emerging technology that involves the use of CT data at two different energy levels (e.g., 80 kVp and 140 kVp).The characteristic attenuation patterns of different materials at these different energy levels provide advantages that are not available from traditional single energy CT, such as the improved ability to evaluate the distribution and density of various chemical elements[23].One study measured lung cancer tissue of different pathological types and found that lung squamous cell carcinoma had the highest concentration of calcium, followed by lung adenocarcinoma,large cell lung cancer,and small cell lung cancer(p<0.05).Calcium-based material images are very sensitive to calcium deposition.Therefore, it can be used for the determination of tissue calcium content.Ureteral stones cause persistent irritation, even up to 3 years in our cases, that leads to edema and fibrosis in the ureter mucosa.Pathologic studies have shown the occurrence of chronic interstitial fibrosis and urothelial hypertrophy at the point in the ureteral lesion.Decreased blood flow due to prolonged physical pressure or an immunological response to stones causes chronic inflammation at the ureter mucosa[13,24-26].We believe that with chronic inflammation and fibrosis, ureteral smooth muscle cells with a calcium pool may be replaced by fibrous tissue, which is the reason that the calcium concentration of the ureter in the hardening group is significantly lower than that in the other groups.In addition,with the aggravation of chronic inflammation,the adhesion between the ureter and stone is more serious,which leads to the aggravation of hydronephrosis.In this study, hydronephrosis was associated with ureteral hardening [27,28].
The literature showed obvious controversies regarding risk factors for post-URSL stricture.Early studies were retrospective with a short follow-up[4].Early research by Roberts et al.[29], Brito et al.[9], and Devarajan et al.[30] discovered that ureteral perforation at the site of the stone, damage to the mucous membrane, and leftover stones lodged within the ureter mucosa were identified as risk factors for stricture formation.However,some prospective studies in recent years suggest that these factors are not risk factors for ureteral stricture.The reason for the different conclusions may be due to the upgrade of surgical equipment, such as the diameter of the ureteroscope and application of holmium laser.Notably, the majority of these studies, whether early or recent, agreed that impacted stone is the most common cause of ureteral stricture after URSL surgery [4,13,29].Therefore, ureteral lesions around the impacted stone are extremely important for predicting postoperative ureteral stricture.
Yoshida et al.[31] pointed out that high UWT is associated not only with a higher risk of impacted stones but also with ureteral lesions.However,we found that some lesions of the ureter around the stone were almost invisible on CT.In our experience, ureteral lesions occur not only around the stone but also at its upper and lower margins.Therefore, the UWT and DECT parameters were measured close to the lower edge of the stone.Unlike previous studies,we found that UWT is not associated with ureteral lesions.The reason for the different results could be that the patients in our study all had impacted stones,while the previous study included non-impacted calculi.
In general,larger stones put more pressure on the ureter and increase the risk of ureteral stricture.In a retrospective study by El-Abd et al.[8], the postoperative ureteral stricture rate was 4.4% in patients with calculi larger than 2 cm, while only 0.2% of patients with calculi smaller than 2 cm had strictures.However, in two prospective studies,Fam et al.[13] and Darwish et al.[4] found that there was no significant correlation between the size of ureteral stones and postoperative stricture.In this study, we obtained the same results.
According to Weizer et al.[32], silent ureteral stricture may occur in 2.9% of patients after URL and has a greater potential risk for patients.Patients may experience a decline in renal function without symptoms, which can eventually lead to kidney loss.For these patients, the calcium concentration of the ureter can be used to identify ureteral hardening and to make a more comprehensive follow-up plan.Some studies recommended at least 18 months of follow-up in patients with risk factors for ureteral stricture [8].
There are some shortcomings in this study.First, the number of ureteral strictures is small, and the sample size should be increased for further analysis.Second, patients have not received follow-up in a longer time after surgery,so that it is possible to cause detection bias.Third, no pathological examination of ureteral hardening tissue was conducted in this study.Fourth, during follow-up of the patients, the detection of residual stones by ultrasound may be missed.Finally,the study is of observational nature and the proposed cut-off was made post hoc.
Despite of limitations existed, this study can still promote researches on how to determine surgical methods based on different ureteral lesions.
5.Conclusion
The calcium concentration of the ureter is an independent predictor of ureteral hardening.Hydronephrosis after URSL in patients with ureteral hardening was worse than in those without ureteral hardening.A calcium concentration value of 5.3 mg/cm3was the optimal cut-off value.When the calcium concentration of the ureter is less than 5.3 mg/cm3, ureteral hardening should be actively treated after URSL to reduce the risk of postoperative ureteral stricture and maximize the protection of renal function.
Author contributions
Study concept and design: Qilin Xi, Junjie Wang.
Data acquisition: Junjie Wang, Ximing Wang, Haozhou Zhong, Wengui Xie.
Data analysis: Junjie Wang.
Drafting of manuscript:Junjie Wang.
Critical revision of the manuscript: Qilin Xi.
Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2023年4期
Asian Journal of Urology2023年4期
- Asian Journal of Urology的其它文章
- Robot-assisted adrenalectomy: Step-by-step technique and surgical outcomes at a high-volume robotic center
- The application of internal suspension technique in retroperitoneal robot-assisted laparoscopic partial nephrectomy with a new robotic system KangDuo Surgical Robot-01: Initial experience
- A systematic review of robot-assisted partial nephrectomy outcomes for advanced indications: Large tumors (cT2-T3), solitary kidney, completely endophytic, hilar,recurrent, and multiple renal tumors
- Three-dimensional automatic artificial intelligence driven augmented-reality selective biopsy during nerve-sparing robot-assisted radical prostatectomy:A feasibility and accuracy study
- First 100 cases of transvesical single-port robotic radical prostatectomy
- Robot-assisted oncologic pelvic surgery with Hugo?robot-assisted surgery system: A single-center experience