
Electrophysiological evaluation of alterations in penile sensation due to penile prosthesis implantation in patients with erectile dysfunction
2024-01-11 11:02irhimErolAlildKnKrmHknAnEkremIslmogluTuncyMutluAtesMurtSvs
Asian Journal of Urology 2023年4期
irhim Erol *, Ali Y?ld?z Kn Krm?k Hkn An?l Ekrem.Islmo?glu Tuncy C?k?r , Mutlu Ates? Murt Svs?
a Department of Urology, Antalya Training and Research Hospital, University of Health Sciences,Antalya, Turkey
b Department of Physical Medicine and Rehabilitation, Antalya Training and Research Hospital,University of Health Sciences, Antalya, Turkey
KEYWORDS Penile prosthesis;Penile sensation;Electromyography;Erectile dysfunction
Abstract Objective: The present study was aimed to determine the effect of penile prosthesis implantation (PPI) surgery on penile sensation by evaluating the penile electromyography (EMG) variables.Methods: The research was designed as a prospective study.Thirty patients who were diagnosed with organic erectile dysfunction and had underwent PPI surgery between January 2017 and January 2018 in the Urology Clinic of Antalya Training and Research Hospital were included in this study.Penile sensory EMG was performed on each patient 1 day prior to the surgery by the Physical Therapy and Rehabilitation clinic.Additionally, the control EMG study was also performed in the 3rd and 6th postoperative months.Results: We included 27 patients in this study who attended regular follow-ups and had complete EMG results.Out of the 27 patients,23(85.2%) patients had received malleable (ProMedon)penile prosthesis,one(3.7%)patient had received a two-piece inflatable(Ambicor)penile prosthesis, and three (11.1%) patients had received a three-piece inflatable (AMS 700 CXR)penile prosthesis.The mean nerve conduction value(NCV)of the patients was 29.85(standard derivation: 22.54; range: 0-78.4) m/s during the preoperative period, whereas it was 27.64(standard derivation: 24.72; range: 0-83.3) m/s in the 3rd postoperative month and 24.80(standard derivation: 22.31; range: 0-88.4) m/s in the 6th postoperative month.There was no significant difference between preoperative NCV and 3rd postoperative month NCV(p=0.607).Similarly, no significant difference was observed between preoperative NCV and 6th postoperative month NCV (p=0.276).Additionally, the change between NCV values at postoperative 3rd and 6th months was not statistically significant (p=0.553).Conclusion: Significant loss of penile sensation does not occur in patients who undergo PPI surgery.
1.Introduction
Erectile dysfunction (ED) is defined as persistent inability in men to achieve and maintain an adequate erection that does not allow satisfactory sexual performance [1-3].According to the guidelines of the European Association of Urology,the etiologies of ED are reported under six main categories that include vascular, anatomical or structural, neurogenic,hormonal, psychogenic, and medication-related causes [1].Treatment with penile prosthesis implantation (PPI) surgery is considered as an ultimate treatment option in patients who fail to respond to the first-and second-line of treatment of ED [2].
PPI,which renders high patient and partner satisfaction,is an invasive but effective treatment modality that is frequently used in the treatment of ED.In the literature,there are several techniques and researches that are used to evaluate ED, and electrophysiological evaluation is one such technique[3,4].In PPI surgery,the corpus cavernosum tissue of the penis is dilated with bougies due to which the corpus cavernosum is rendered irreversibly dysfunctional.The effect of the trauma during the surgery and the subsequent fibrosis may affect the dorsal nerve adjacent to the corpus cavernosum and reduce penile sensation [5].The electromyography (EMG) can be used to understand whether the nerve damage does affect the penile sensation after the PPI surgery.In this study, we wondered whether PPI reduces penile sensation or not, and we aimed to determine it with penile EMG.
2.Patients and methods
The study was initiated with 30 patients who were diagnosed with organic ED and scheduled for PPI surgery between January 2017 and January 2018 in the Urology Clinic of Antalya Training and Research Hospital,Antalya,Turkey.Patients with persistent organic ED who had not responded to conservative treatments for at least 1 year and who volunteered to participate in PPI treatment with normal hormonal levels (testosterone, thyroid function tests, and prolactine) were included in our study.These patients volunteered and provided consents to participate in the study.The present study protocol was reviewed and approved by the Institutional Review Board of Antalya Training and Research Hospital (ethics committee number:2017-018).Informed consents were obtained by all participants when they were enrolled.Patients with high comorbidity that could not have PPI, with trauma or major penile surgery, with severe neurological disease or uncontrolled diabetes (peripheral neuropathy, spinal cord injury, etc.), and who used drugs that could affect the autonomic nervous system such as anticholinergic were excluded from the study.Two participants who did not want to continue were excluded from the study.
The penile sensory EMG was performed on each patient 1 day prior to the surgery by the Physical Therapy and Rehabilitation clinic.A follow-up EMG was performed on the patients in the 3rd and 6th postoperative months.The same surgeon(Dr.Erol)performed the PPI surgery of all the patients with the same incision penoscrotal technique.All steps of the study were conducted inthe Urology and Physical Therapy and Rehabilitation clinic within the Antalya Training and Research Hospital, and were executed by a single researcher in each unit.

Figure 1 Penile electromyography.
Electrophysiological studies were carried out in accordance with the Clawson method(Fig.1)[3,4].A two-channel electroneuromyography device (Nihon-Kohden-Neuropack,model MEB-2200-Tokyo, Japan) was used for recording.In this method, the penis was placed in the concavity of especially designed Orthoplast penile traction device (this device is produced from hospital supplies abeslang, cunningham incontinence clamp, etc.) and it was stretched to reach its maximum length by holding the tip of the glans.The Cunningham incontinence clamp(Biyoclamp, Melikgazi,Kayseri, Turkey) was attached to the glans, and the glans continued to be held with the penis stretched.Electroencephalography cream was applied and steel electrodes were placed as active and reference electrodes.The active recording electrode was placed as adjacent as possible to the root of the penis proximally.The reference electrode was placed 4 cm above the active electrode.For the purpose of recording the data, orthodromic stimulations were transmitted using the active electrode from the proximal to the dorsal aspect of the penis, and using the reference electrode to the dorsal glans penis [3].
In the descriptive statistics of the data, mean, standard deviation, median, lowest, highest, frequency, and ratio values were used.The distribution of variables was assessed using the Kolmogorov-Smirnov test.Mann-Whitney U test was used to analyze the quantitative independent data.SPSS 24.0 (IBM SPSS Statistics, New York, NY, USA) program was used for data analysis, and p<0.05 was considered as significant.
3.Results
Out of the 30 patients initially included in the study, one was excluded due to a need for PPI revision and two others were excluded as they were not interested in continuing their follow-ups and participating in the study due to social reason and transportation difficulty.Thus the study was completed with 27 patients.The demographic data of the patients are shown in Table 1.
The patients experienced no complications during the surgery; however, 4 (14.8%) patients did develop complications during a mean±standard deviation (SD) postoperative follow-up of 13±5 (range: 6-24) months.In one (3.7%)patient,the penile prosthesis was removed due to migration and urethral trauma after the PPI surgery.Penile and scrotal hematoma developed in two (7.4%) patients, but tight dressing, scrotal elevation, and antibiotic treatment effectively helped the hematoma to regress and heal during the follow-up period.Furthermore, superficial wound site infection developed in one (3.7%) patient, who also completely recovered with conservative follow-up and antibiotic treatment.
To assess the patients’ the nerve conduction value(NCV) results obtained through the EMG, the lower limit value is generally accepted as 29.8 m/s to evaluate the results of NCV obtained by EMG [4].We found that NCV values of 12(44.4%)patients were below the lower limit of 29.8 m/s preoperatively; 15 (55.6%) and 16 (59.3%) patients had their NCV values below the lower limit in the 3rd postoperative month and 6th postoperative month,respectively.The mean±SD NCV value during the preoperative period was 29.85±22.54 (range: 0-78.4) m/s,whereas the values were 27.64±24.72(range:0-83.3)m/s and 24.80±22.31 (range: 0-88.4) m/s in the 3rd and 6th postoperative months, respectively.It was observed that the mean NCV values during the preoperative period and the 3rd and 6th postoperative months were gradually decreasing.This means that the sensation of the penis was gradually decreasing in the 3rd and 6th postoperative months as compared with the preoperative period.However, the mean values of preoperative NCV andpostoperative values NCV were compared and there was no significant difference observed (Table 2).
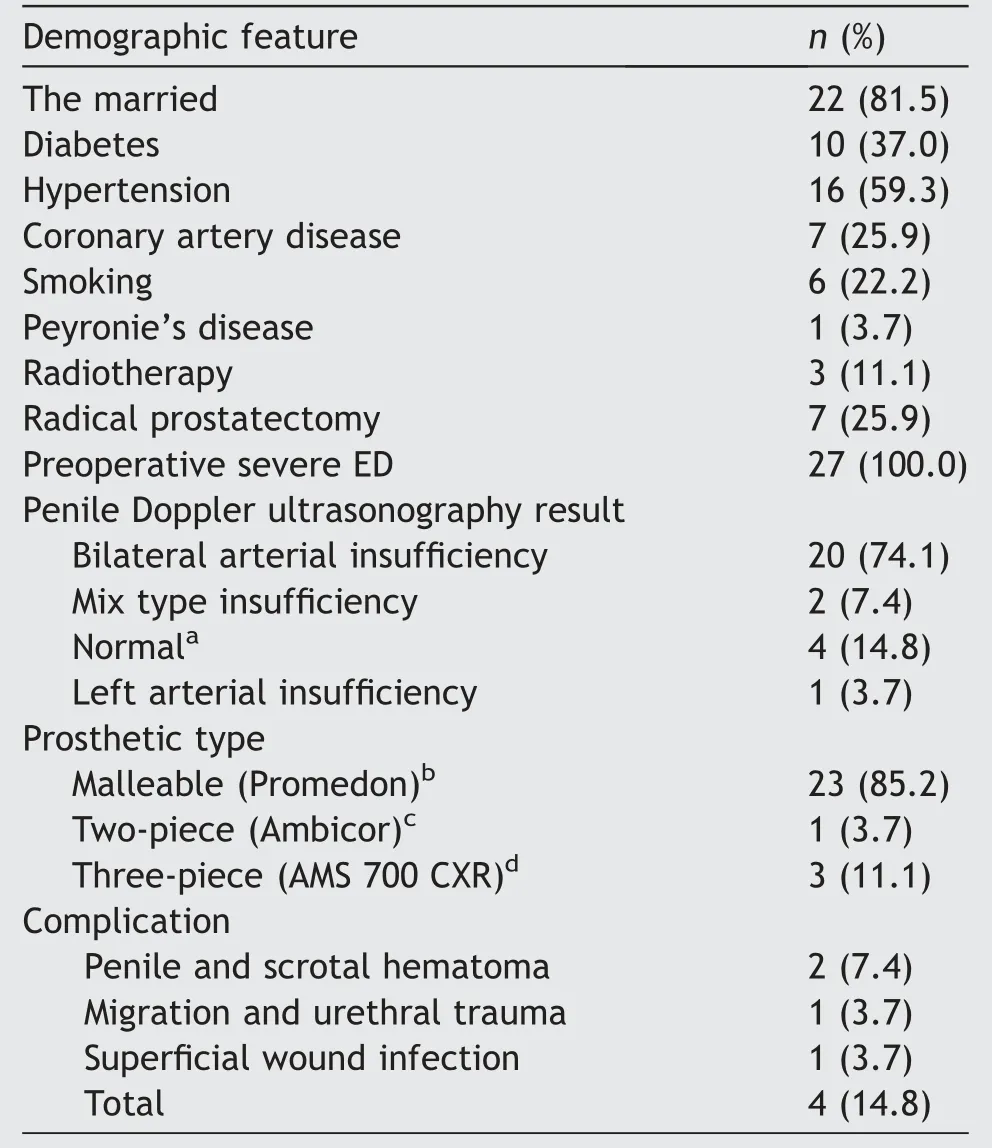
Table 1 Demographic characteristics of patients.
4.Discussion
PPI surgery is an effective treatment option for patients with ED who fail to respond to pharmacological agents[6,7].Despite being an effective treatment option with a high patient satisfaction rate,PPI surgery only accounts for approximately 1% of the opted treatment methods due to its invasive nature [7,8].
It is worthy to note that in cases of patient dissatisfaction with penile prosthesis and its subsequent removal due to the dissatisfaction or any other reasons, the other modalities of ED treatment become ineffectual.Hence,penile prosthesis surgery is opted as the last option in the treatment of ED.Moreover, in PPI surgery, all the cavernous structures are destroyed and natural erection of the penis cannot be achieved.Damage to the cavernous structures induces cavernous nerve damage [9].The dorsal nerve innervates the glans penis, while the branches of the dorsal nerve also extend ventrolaterally through the glans toinnervate the frenulum along with one branch of the perineal nerve;in addition to innervating the glans,it also plays a role in the sensory function of the glans[10-12].Although penile prosthesis surgery does not directly damage the penile sensory innervation, it might cause damage to the dorsal nerve via thermal (using cautery) injury during plug cavernous dilatation or subsequent fibrosis as a result of the cavernosal injury because of its proximity to the prosthesis(especially infrapubic surgery) [7,13].To our knowledge,there is no study in the literature demonstrating loss of penile sensation due to isolated PPI surgery [5,14].
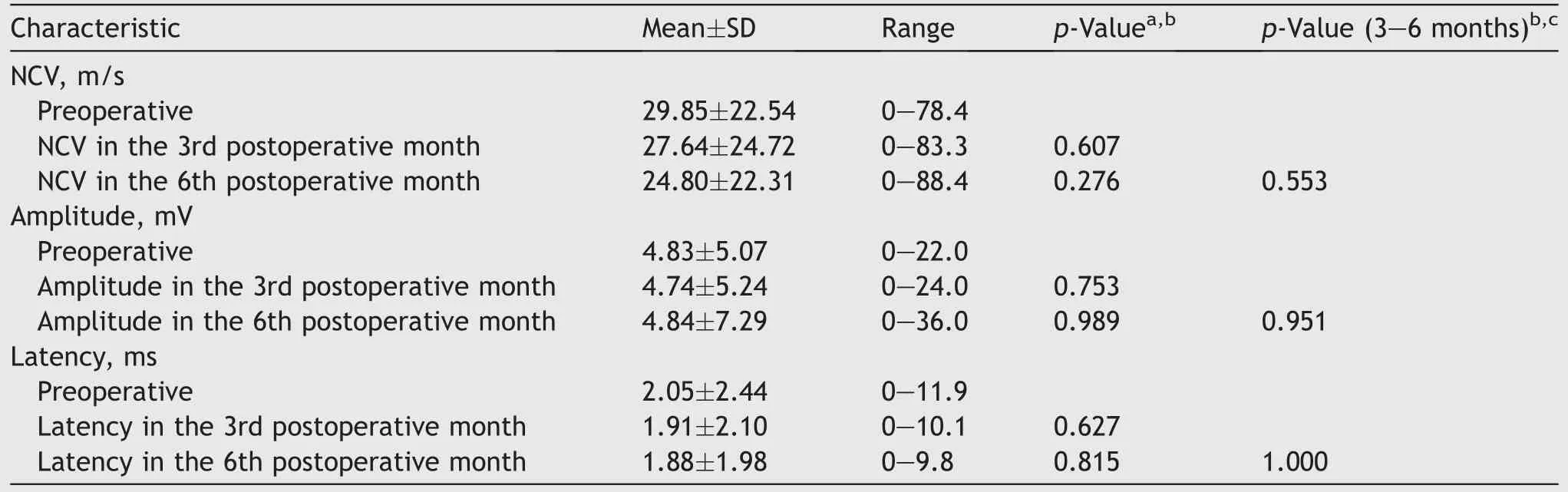
Table 2 Comparison of EMG values (biothesiometer) (n=27).
A study by Soylu et al.[15]compared preoperatively-and postoperatively-stimulated and spontaneous penile electrodermal activity in 10 patients who underwent PPI surgery.They reported that the mean±SD amplitude of stimulated electrodermal activity was reduced from 2159±700 mV to 1413±515 mV following penile prosthesis surgery (p=0.017) [15].Thus, it has been demonstrated that penile autonomic innervations reduces as a result of PPI surgery; however, it does not cause penile sensory loss as it plays no role in the sensory innervation of the penis.
As demonstrated in our study,PPI does not impair penile innervation (there is no dorsal nerve damage) and hence causes no alteration in penile innervation or sensation.However,in a study by Sansalone et al.[16], four out of 20 patients complained of decreased sensation in the glans penis after the PPI surgery.Similarly, there are case presentations in the literature reporting loss of sensation after the PPI surgery [15,16].However, the patients included in their study group were patients with Peyronie’s disease and severe ED requiring additional procedures such as fibrous plaque removal and graft placement.
Xie et al.[5] performed penile sensation measurements on 62 patients with penile prostate using glans or elbow biothesiometer during the preoperative period, the 6th postoperative week, and the 6th postoperative month.They demonstrated that there was no significant sensory loss before and after the surgery [5].Currently, there are no studies which report penile sensation impairment in patients who have only ED and have undergone PPI.Therefore, as demonstrated in our study,we conclude that PPI surgery does not affect penile sensation[5].Thus,with the help of EMG,more objective results can be obtained by quantitating these data.
The pudendal somatosensory stimulation and bulbocavernosus reflex stimulation are the well-defined and conventional electrodiagnostic techniques used for evaluation of patients with ED.Neither of the two above-mentioned methods measures peripheral sensory nerve function.The dorsal nerve of the penis is the terminal sensory branch of the pudendal nerve and transmits sensory data from the glans and shaft of the penis[17-19].The tactile stimulation of the penis and sensory input play an important role in the erection and sexual function of the penis.Some studies have shown that interruption to this input causes loss of libido,ejaculation function, and erection [20,21].Therefore, it is important to accurately measure the function of the dorsal nerve of the penis in evaluating patients with ED.Evaluation of the dorsal nerve of the penis to assess the ED is the valuable diagnostic method considering that it evaluates sensory nerve function and is noninvasive [3].However,measuring NCV, the sensory nerve action potential of the dorsal nerve of the penis, can be a valuable tool in evaluating ED[4].In addition,this method can determine whether there is loss of sensation in the dorsal nerve of the penis,thereby differentiating between neurogenic ED (caused by peripheral neuropathy) and vascular ED [3,4].
Bradley et al.[3]performed EMG studies to evaluate the penile sensation.In the study, certain weights were attached to the tip of the penis and the penis was pulled and elongated.They calculated the NCV at three different instances,i.e.,without weights,with a weight of 1 kg,and a weight of 2 kg.The mean±SD NCV was 27.20±1.65 m/s without weights,31.00±0.88 m/s with a weight of 1 kg,and 31.60±0.83 m/s with a weight of 2 kg in healthy men.As the weight increases,the penis will stretch and lengthen.In this study, it was seen that the lengthening of the penis by pulling increased the NCV value.As a result, the study showed that stretching the penis during shooting was necessary for accurate measurement [3].
Later, this method was modified by Clawson et al.[4] in another study; they standardized the process of stretching the penis with a new equipment that they had developed,and obtained more accurate results by fixating the penis with a penis clamp.In addition,the dependence on gravity was prevented and the difference in length that could be caused by the friction force was overcame.The study reported that the latency values of the patient remained constant(even though the distance between the electrodes changed)and only the NCV values changed[5].We used the method described by Clawson et al.[4]in our current study.
The lower limit value was considered 29.8 m/s while assessing Clawson’s NCV results obtained through EMG [19].Since all the patients included in our study were diagnosed with ED,the mean NCV value was below the lower limit value even prior to the surgery.Of all the EMG parameters,NCV was the best parameter that demonstrates sensory loss.In addition, although the mean NCV values decreased gradually during the preoperative period and in the 3rd and 6th postoperative months,they were numerically close to each other and thus the decrease was not statistically significant[3,4].
The most important limitation in our study is the low number of patients (n=27).Therefore, it cannot be generated to the whole society.Further studies with more number of patients are warranted to better understand the effect of PPI surgery on penile sensation in order to derive definitive results.
5.Conclusion
In this study, we aimed to determine if penile prosthetic implantation with a high rate of satisfaction reduces penile sense.We observed that there was a slight reduction in the mean values of all EMG parameters (NCV, latency,and amplitude)after the surgery,but this reduction was not statistically significant (p>0.05).Thus, we have quantitatively demonstrated that PPI surgery does not affect penile sensation.
Author contributions
Study concept and design:.Ibrahim Erol, Ali Y?ld?z, Kaan Karam?k, Hakan An?l.
Data acquisition: Ekrem.Islamo?glu, Tuncay C?ak?r, Mutlu Ates?, Murat Savas?.
Data analysis: Kaan Karam?k, Hakan An?l, Ekrem.Islamo?glu,.Ibrahim Erol.
Drafting of manuscript: Tuncay C?ak?r, Mutlu Ates?,.Ibrahim Erol.
Critical revision of the manuscript: Mutlu Ates?, Murat Savas?,.Ibrahim Erol.
Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2023年4期
Asian Journal of Urology2023年4期
- Asian Journal of Urology的其它文章
- Robot-assisted adrenalectomy: Step-by-step technique and surgical outcomes at a high-volume robotic center
- The application of internal suspension technique in retroperitoneal robot-assisted laparoscopic partial nephrectomy with a new robotic system KangDuo Surgical Robot-01: Initial experience
- A systematic review of robot-assisted partial nephrectomy outcomes for advanced indications: Large tumors (cT2-T3), solitary kidney, completely endophytic, hilar,recurrent, and multiple renal tumors
- Three-dimensional automatic artificial intelligence driven augmented-reality selective biopsy during nerve-sparing robot-assisted radical prostatectomy:A feasibility and accuracy study
- First 100 cases of transvesical single-port robotic radical prostatectomy
- Robot-assisted oncologic pelvic surgery with Hugo?robot-assisted surgery system: A single-center experience