
Can preoperative planning using IRIS?three-dimensional anatomical virtual models predict operative findings during robot-assisted partial nephrectomy?
2024-01-11 11:02AhmedGhziNitinShrmAhmedRdwnHniRshidThomsOsinskiThomsFryeWillimTyoyongJonthnBloomJenJoseph
Asian Journal of Urology 2023年4期
Ahmed Ghzi , Nitin Shrm ,*, Ahmed Rdwn ,Hni Rshid , Thoms Osinski , Thoms Frye ,Willim Tyoyong , Jonthn Bloom , Jen Joseph
a University of Rochester, Urology Department, Rochester, NY, USA
b Ain Shams University, Urology Department, Cairo, Egypt
KEYWORDS Renal cancer;Patient-specific;Three-dimensional virtual model;Imaging;Partial nephrectomy;Robotics
Abstract Objective: To evaluate the predictive validity of IRIS?(Intuitive Surgical?,Sunnyvale, CA, USA) as a planning tool for robot-assisted partial nephrectomy (RAPN) by assessing the degree of overlap with intraoperative execution.Methods: Thirty-one patients scheduled for RAPN by four experienced urologists were enrolled in a prospective study.Prior to surgery,urologists reviewed the IRIS?three-dimensional model on an iphone Operating System (iOS) app and completed a questionnaire outlining their surgical plan including surgical approach,and ischemia technique as well as confidence in executing this plan.Postoperatively, questionnaires assessing the procedural approach, clinical utility,efficiency, and effectiveness of IRIS?were completed.The degree of overlap between the preoperative and intraoperative questionnaires and between the planned approach and actual execution of the procedure was analyzed.Questionnaires were answered on a 5-point Likert scale and scores of 4 or greater were considered positive.Results: Mean age was 65.1 years with a mean tumor size of 27.7 mm(interquartile range 17.5-44.0 mm).Hilar tumors consisted of 32.3%; 48.4% of patients had R.E.N.A.L.nephrometry scores of 7-9.On preoperative questionnaires,the surgeons reported that in 67.7%cases they were confident that they can perform the procedure successfully,and on intraoperative questionnaires,the surgeons reported that in 96.8%cases IRIS?helped achieve good spatial sensation of the anatomy.There was a high degree of overlap between preoperative and intraoperative questionnaires for the surgical approach, interpreting anatomical details and clinical utility.When comparing plans for selective or off-clamp, the preoperative plan was executed in 90.0% of cases intraoperatively.Conclusion: A high degree of overlap between the preoperative surgical approach and intraoperative RAPN execution was found using IRIS?.This is the first study to evaluate the predictive accuracy of IRIS?during RAPN by comparing preoperative plan and intraoperative execution.
1.Introduction
The incidence of renal cell carcinoma (RCC) especially for localized disease has significantly increased from 3.7 to 7.0 cases per 100 000 United States adults in the last decade with the widespread utilization of cross-sectional imaging[1,2].The standard treatment for such clinical tumor stage 1(cT1)and cT2 RCC is nephron-sparing surgery[3,4].With the advancement in minimally invasive surgical techniques, robot-assisted partial nephrectomy (RAPN) has become the preferred treatment modality for such renal masses [5].Along with surgeon’s experience, success of RAPN depends on meticulous review of two-dimensional(2D) computed tomography (CT) and magnetic resonance imaging to formulate various approaches to RAPN including type of ischemia based on tumor size, tumor location and its relation to renal vessels and collecting system.Surgical complexity of partial nephrectomy is also assessed by various tools such as R.E.N.A.L.nephrometry scores and Preoperative Aspects and Dimensions Used for Anatomical(PADUA)classification scores,which are directly dependent on preoperative imaging [6,7].Therefore, providing urologists with high-quality imaging in a format that is most conducive towards optimizing the decision making and intraoperative execution of the planned procedure plays a critical role.
The increasing popularity of segmentation softwares with the capability of transforming Digital Imaging and Communications in Medicine (DICOM) files into three-dimensional virtual reconstructions(3D-VRs)has aided urologists in performing precision surgery for various urogenital malignancies[8].RCCs are particularly suitable for precision surgery, as nephron-sparing surgery is highly dependent on the inherent tumor pathology and renal vascular anatomy,all of which are enhanced via 3D reconstructions[8].
Over last decade,several studies have demonstrated the clinical utility of 3D-VR for RAPN with improved surgical outcomes [9-12].However, few if any have demonstrated the overlap between the preoperative plan and intraoperative execution, i.e., the ability of 3D-VR to predict intraoperative findings (predictive validity).
In this study, we utilized IRIS?, an interactive 3D-VR software along with 2D CT scan to evaluate its clinical utility in RAPN.IRIS?is a modelling software developed by intuitive(Intuitive Surgical?, Sunnyvale, CA, USA) to provide 3D-VR images of the renal anatomy and pathology.The platform has an interactive interface allowing functional manipulation of the 3D images(e.g.,altering transparency,rotating,zooming, and panning).In a previous premarket study, we have assessed the fidelity of IRIS?platform and how it influenced surgeons’confidence in the decision-making process[13].In this study, we evaluated the clinical utility and fidelity of IRIS?in preoperative planning of RAPN as well as the degree of overlap between the preoperative assessment or plan and the actual intraoperative findings or execution during RAPN utilizing the IRIS?.
2.Patients and methods
2.1.Study design (Fig.1)
In this prospective single-center post-market study, 31 patients diagnosed with cT1 and cT2 localized renal tumors were included (from September 4th, 2020 to December 30th, 2021) following institutional review board approval(STUDY00004707).Based on the power analysis performed in our initial retrospective study, the sample size of patients for IRIS?was calculated to be a minimum of 30 patients [13].Based on exclusion and inclusion criteria(Table 1), patients were enrolled in the study and appropriate informed consent was obtained from each patient.Complex cases like those with horseshoe kidney or multiple lesions were intentionally excluded from the study to allow for a comparative analysis.Patient demographics, relevant clinical history,disease characteristics,clinical staging and R.E.N.A.L.nephrometry scores were recorded for each case based on CT imaging (Table 2).Intuitive Surgical was provided with patient’s CT scans in DICOM format through a Health Insurance Portability and Accountability Act(HIPAA)compliant picture archiving and communications system(PACS)server to reconstruct a patient specific 3D-VR model that was viewed by the urologists using an app installed on an iphone Operating System (iOS) device (Apple Park,Cupertino, CA, USA) (Fig.2).Urologists first reviewed the 3D-VR IRIS?model prior to completing preoperative questionnaires assessing the usefulness of the technology in the interpretation of anatomy, confidence in performing RAPN and RAPN approach, and degree of ischemia.During RAPN,intraoperative navigation was performed using IRIS?model within the da Vinci surgeon console using TilePro.Postoperatively, urologists completed another set of questionnaires to evaluate the impact of IRIS? on actual intraoperative anatomy, procedure efficiency, and ease of utility of IRIS?.The degree of overlap between the preoperative and intraoperative questionnaires as well as between the planned clamping technique and the actual clamping performed intraoperatively was evaluated.Patients were assessed postoperatively at 14 days and 90 days to evaluate for postoperative outcomes.Operative outcomes like operation room time,expected blood loss(EBL),transfusion requirement during surgery, type of clamping(off-clamp, primary renal artery, selective, or superselective), and clamping time were noted in each case.Postoperative outcome variables like intensive care unit requirement, length of hospital stay, pathology, margin status, and complications were noted.

Figure 1 Study design.CT, computed tomography; MRI, magnetic resonance imaging; DICOM, Digital Imaging and Communications in Medicine; 3D, three-dimensional; EBL, expected blood loss; iOS, iphone Operating System.

Table 1 Inclusion and exclusion criteria for the study.
2.2.Statistical analysis
Questionnaires were designed to evaluate various preoperative and intraoperative variables like surgeon’s confidence in completing the procedure,interpretation of anatomy and sufficiency of information, on a 1-5 Likert scoring system and the percentage of reviews receiving a score of ≥4 was calculated.The degree of agreement between the preoperative and intraoperative variables was measured by the percentage of overlap between these two variables.To evaluate the difference in intraoperative and preoperative assessment on IRIS?, agreement analysis was performed using the Bland-Altman analysis,which is a statistical tool to assess the degree of agreement between two quantitative methods of measurement [14].A 95% confidence intervalSD,standard deviation;IQR,interquartile range;BMI,body mass index;ASA,American Society of Anesthesiologists;LOS,length of stay.
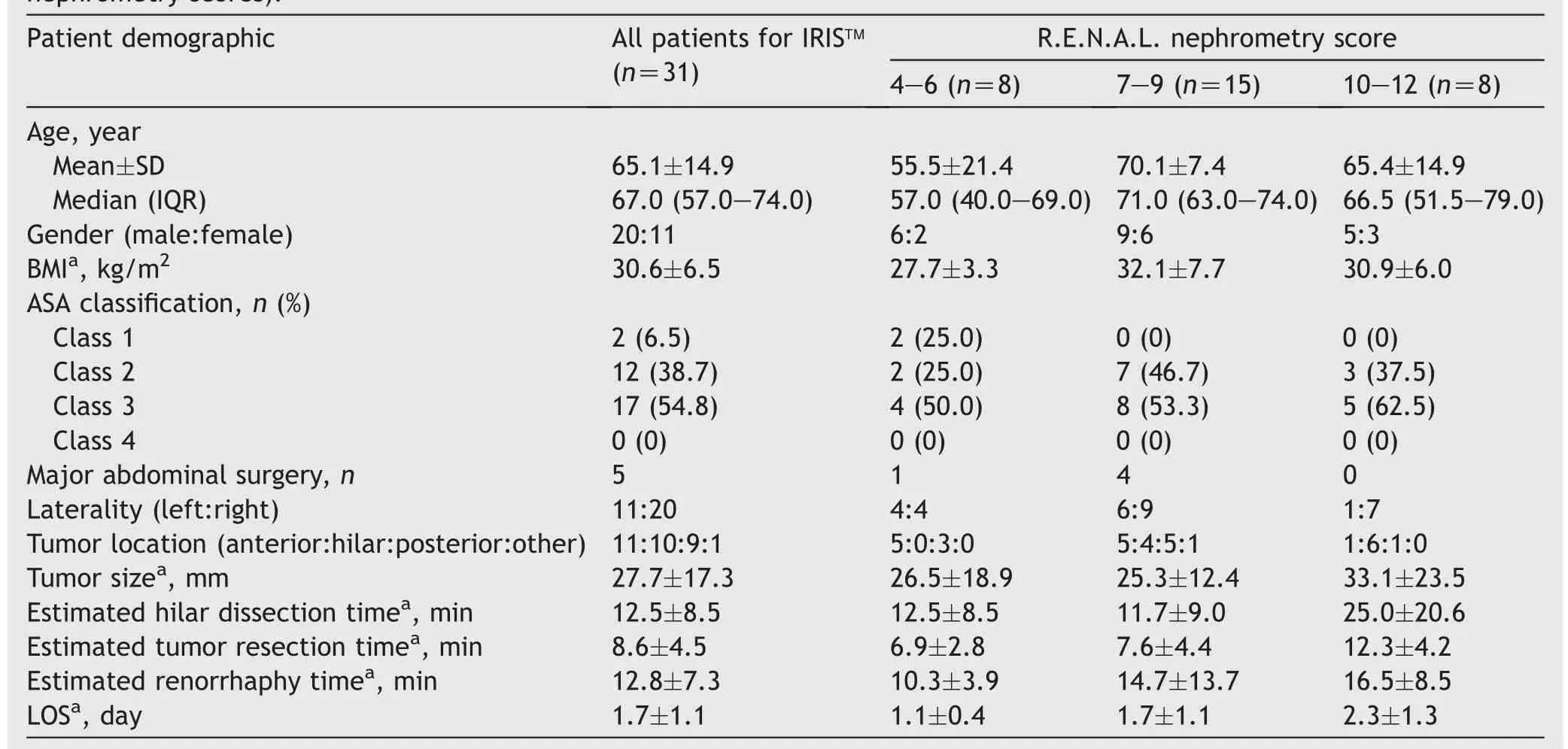
Table 2 Patient demographics, medical and surgical history, and surgical outcomes (grouped according to R.E.N.A.L.nephrometry scores).
aValues are presented as mean±SD.was calculated by evaluating the average of difference between the preoperative and intraoperative questionnaires and Bland-Altman plot was constructed.

Figure 2 A patient with a complex left renal mass(R.E.N.A.L.nephrometry score of 10).(A) Coronal images of abdominal computerized tomography scan; (B) IRIS?three-dimensional virtual reconstruction image on iphone Operating System device(Apple Park, Cupertino, CA, USA) of the same patient.R, right;L, left.
3.Results
A total of 31 patients were classified into three groups depending on the complexity of the case based on the R.E.N.A.L.nephrometry score (4-6, 7-9, and 10-12).Patients had a mean age of 65.1 years, and mean body mass index of 30.6 kg/m2; 17 (54.8%) patients had an American Society of Anesthesiologists Class 3.Mean tumor size was 27.7 mm (interquartile range 17.5-44.0 mm).Hilar tumors consisted of 32.3%; 48.4% of patients had R.E.N.A.L.nephrometry scores of 7-9 (Table 2).
On preoperative planning questionnaires, 100% of surgeons reported a Likert scoring system score of 4 or higher for facilitating interpretation of anatomy,and the surgeons reported that in 67.7% cases they were confident in performing a RAPN successfully after reviewing the IRIS?model (Table 3).Less than or equal to 5 min was spent in reviewing the IRIS?model in 90.3%of cases with only three cases requiring more than 5 min for review of 3D-VR model(one with R.E.N.A.L.nephrometry score 4-6; two with R.E.N.A.L.nephrometry scores 7-9).All patients underwent transperitoneal RAPN by four experienced urologists.Mean procedure time (skin to skin) was 163.3 min, with mean EBL of 108.8 mL.Mean clamp time was 17.8 min among all patients and was 21.8 min in complex tumors(R.E.N.A.L.nephrometry scores 10-12).Only one patient with an 8 cm posterior hilar tumor with a R.E.N.A.L.nephrometry score of 11 had a clamp time of 31 min.Mean hilar dissection time and tumor resection time was 15.3 min and 8.6 min, respectively.In four patients, pelvicalyceal system violation could not be avoided and repair was required.Primary renal artery clamping was planned preoperatively in 11 cases and was executed in 13 cases with 84.6% overlap (Table 4).Similarly, selective, or off-clamp approach was planned in 20 cases and executed in 18 cases (90% overlap in clamping decision).Further breakdown of selective clamping overlap is detailed in Table 4.None of the patients encountered any ischemic renal or vascular complications in the perioperative period.
Intraoperatively the surgeons reported that in 96.8%cases IRIS?helped achieve good spatial sensation of the anatomy, and ratings reached 100% for higher renal score cases (R.E.N.A.L.nephrometry scores 7-12) (Table 3).All surgeons (100.0%) reported that they found IRIS?model easy to use and interpret and none reported any alteration in intraoperative plan compared to preoperative plan afterusing IRIS? or during intraoperative use (Table 5).Regarding features within the interactive IRIS?interface,the surgeons reported pan and rotation in 87.1%cases,and alternating transparency in 71.0% cases as the most useful features of IRIS?(Table 5).The surgeons reported that in more than 90%cases, IRIS?3D model was beneficial during case discussion with the patient and is a useful tool for teaching trainees (Table 5).Bland-Altman plot was used to compare the degree of agreement between surgeon’s preoperative interpretation of anatomy and pathology for planning and actual intraoperative findings and executed plan, demonstrated a high degree of overlap between intraoperative and preoperative decisions (95% CI:-0.531-1.076) (Fig.3).

Table 3 Preoperative questionnaires given to surgeon.
4.Discussion
Over last two decades, RAPN has decreased the morbidity and complications while maintaining the oncological efficacy of surgical treatment of RCC.Surgical approach and vascular control in RAPN vastly depend on the information provided on imaging, particularly renal vascular anatomy,tumor depth, and most importantly its proximity to the collecting system and vascular structures.Urologists with extensive experience can predict expected intraoperative findings based on their ability to cognitively reconstruct 3D images following review of axial imaging and align them with encountered intraoperative findings.Studies have shown that 3D-VR images obtained using various software technologies, regardless of the type or source can provide improved and more precise anatomical details which can be directly translated into improved partial nephrectomy outcomes even in less experienced hands [9-11,15].
In the past decade, 3D-VR imaging has been obtained utilizing radiological software but lacked widespread adoption due to their cost, lack of reproducibility, and complicated structure.Recent technological advancements have enabled the development of accurate 3D-VR models that are more intuitive, user friendly, and capable of key functional features that allow manipulation of the 3D-VR model by the surgeon.Studies have either evaluated their role in surgical planning or their role in intraoperative guidance and navigation[16].3D-VR models have also beenutilized in patient education and trainee teaching [17] as well as in augmented virtual reality procedures [18,19].In this study, we have attempted to assess the degree of overlap between preoperative interpretation of anatomy and actual intraoperative findings as well as planned clamping technique and actual intraoperative clamping performed.

Table 4 Preoperative predictive accuracy of IRIS?in comparison to intraoperative findings based on comparison of preoperative and intraoperative questionnaires.
The first report using 3D models included fours cases of complex renal masses where the patients’reconstructed 3D images and video clips were presented to the surgeon preoperatively to aid in identifying tumor-specific feeding vessels [20].Surgeons were able to perform off-clamp partial nephrectomy in these cases.This laid the foundation for use of 3D-VR in partial nephrectomy.Following this report,various types of 3D-VR models were used to evaluate their impact on surgical planning and execution of RAPN.
Porpiglia et al.in 2018 [15] performed a comparative study where standard RAPN (in 31 patients) was compared with RAPN after using hyper accuracy 3D-VR models in 21 patients with complex renal masses (PADUA score ≥10).Significantly less global ischemia was seen in 3D group compared to the standard group (80% vs.24%, p<0.01).Moreover, like our study, they showed greater than 90%overlap in preoperative clamping planned and actual clamping performed.In 2019, they also compared complexity of 101 renal masses using PADUA and R.E.N.A.L.nephrometry scores using 3D-VR and conventional 2D images.3D-VR models resulted in downgrading of R.E.N.A.L.nephrometry scores (from 48.5% to 29.7%) and had higher accuracy in predicting overall and major postoperative complications [21].
In 2019, Hyde et al.[22] presented 3D-VR model to 25 fellow urologists and evaluated a questionnaire regarding anatomical structures,surgical approach,and confidence in performing RAPN.Surgeons unanimously stated that 3D-VR models were of great benefit,changed surgical approach in 19%of cases and were able to perform segmental clamping in 4/5 patients.
Shirk et al.[10] in 2019 reported results from a case control study where he used a 3D-VR model which is viewed on both surgeon’s smartphone and in immersive virtual reality using cardboard headset.Main limitations of the study were that the intervention group(CT in addition to 3D group) and control group were not comparable, and there was no significant difference in clamp time,EBL,or hospital stay between both groups without controlling for case complexity.Shirk et al.[11]later performed a multicentric case control prospective study with 92 patients.The study lacked uniformity due to involvement of 11 surgeons with different levels of experience including trainees (fellows and residents) in more than half cases.On reviewing the literature,we realized that most of these studies have tried to investigate the difference in operative outcome with and without the use of 3D-VR models and have not found any significant difference in the surgical outcome.When controlling for case complexity, use of 3D-VR was found toimprove outcome in complex partial nephrectomy, by significant decrease in the ischemia time.
Most studies have used 3D models viewed using a complex delivery platform requiring specialized setup or dedicated operating personnel, whereas IRIS? provides a user-friendly technology that synchronizes with an intuitive iOS device offering a variety of interactive, functional features, like panning and transparency, providing more detailed anatomical delineation that are directly intergraded into the robotic surgical console intraoperatively using the built-in TilePro feature.
Very few questionnaire-based studies have been attempted assessing the surgeon’s confidence and his understanding of the anatomical structures based on visualization of 3D-VR models [22,23].Antonelli et al.[23] have compared conventional CT scan with 3D holographic reconstructions and have shown high level of interobserver agreement and shorter evaluation time using 3D-VR models.Checcucci et al.[24]evaluated surgeon’s perception of the utility of these models in preoperative surgical planning in complex renal masses.Surgeons highly rated these models for preoperative accuracy and for planning their renography.Secondly after reviewing the model, there was 64.45%change in clamping technique and 44.45%change in resection strategy.
In our study, we have realized there is a high degree of overlap between the preoperative assessment and intraoperative findings using the IRIS?.We have found that use of IRIS?increased surgeon’s confidence in understanding anatomy and hence successful execution of the procedure.The initial result of our study looks promising, particularly in cases where we were able to perform selective or off-clamp RAPN preserving renal function without increase in operative time or vascular complications.

Figure 3 Bland-Altman plot evaluating the difference in intraoperative and preoperative assessment on IRIS?.Orange line indicates the mean difference in questionnaires.95% of the values (blue dot) lie within 2 standard deviation of mean difference in questionnaires.The calculated 95% confidence interval of -0.531-1.076 is suggestive of insignificant or no difference between preoperative and intraoperative response based on the questionnaires.
On evaluating the clinical utility of IRIS?,it was found to be very intuitive, have the potential to improve procedure efficiency, and be beneficial in patient-specific preoperative counselling and resident and/or fellow teaching.IRIS?technology, as any new technology has an initial learning curve, and with more frequent use of this technology,surgeons explore more useful features for applying this technology for improved surgical outcomes.
There are various limitations of our study.This study lacks a control group (planning based on conventional imaging alone) with a relatively small sample size despite being one of the largest single center prospective trials utilizing 3D-VR models for RAPN planning.Further comparative trials are needed to evaluate if all the benefits we have seen using IRIS?result in improved surgical efficiency and hence operative outcomes.We are actively completing a multicenter, prospective case control randomized trial comparing perioperative outcome between patients undergoing RAPN with or without the aid of IRIS?3D model software.
5.Conclusion
This is the first study to assess the predictive validity of the 3D-VR IRIS?technology, i.e., its ability to predict intraoperative findings.The high degree of overlap between the preoperative assessment and intraoperative navigation using IRIS?allowed surgeons to not only confidently plan the procedure but also perform the procedure efficiently with consistency in planning and execution of RAPN procedures.
Author contributions
Study concept and design:Ahmed Ghazi,Rashid Hani,Nitin Sharma, Ahmed Radwan, Thomas Osinski, Thomas Frye,William Tabayoyong, Jonathan Bloom, Jean Joseph.
Data acquisition: Ahmed Ghazi, Nitin Sharma, Ahmed Radwan, Thomas Frye, Hami Rashid, Jonathan Bloom.
Data analysis:Ahmed Ghazi,Nitin Sharma,Ahmed Radwan.Drafting of manuscript: Ahmed Ghazi, Nitin Sharma.
Critical revision of the manuscript: Ahmed Ghazi, Nitin Sharma, Ahmed Radwan.
Conflicts of interest
The study was funded by an industry sponsored research grant from Intuitive Surgical (Sunnyvale, CA, USA).The authors declare no direct conflicts of interest.The sponsor did not influence the design,conduct,or publication of this research.
 Asian Journal of Urology2023年4期
Asian Journal of Urology2023年4期
- Asian Journal of Urology的其它文章
- Robot-assisted adrenalectomy: Step-by-step technique and surgical outcomes at a high-volume robotic center
- The application of internal suspension technique in retroperitoneal robot-assisted laparoscopic partial nephrectomy with a new robotic system KangDuo Surgical Robot-01: Initial experience
- A systematic review of robot-assisted partial nephrectomy outcomes for advanced indications: Large tumors (cT2-T3), solitary kidney, completely endophytic, hilar,recurrent, and multiple renal tumors
- Three-dimensional automatic artificial intelligence driven augmented-reality selective biopsy during nerve-sparing robot-assisted radical prostatectomy:A feasibility and accuracy study
- First 100 cases of transvesical single-port robotic radical prostatectomy
- Robot-assisted oncologic pelvic surgery with Hugo?robot-assisted surgery system: A single-center experience